The Hidden Reality Behind That Silent Bulge in Your Brain
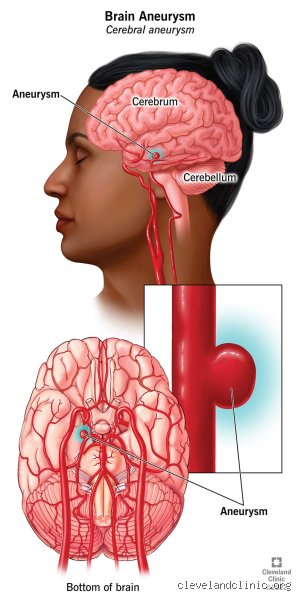
Imagine a tire with a weak spot where the rubber thins out, bubbling outward under relentless pressure until it looks ready to pop during a high-speed highway drive. That is essentially what a cerebral aneurysm is, an abnormal focal dilation of an artery wall caused by a structural weakness in the tunica media. And the thing is, most people walking around with them have absolutely no clue because they rarely cause symptoms until the moment they snap. They are usually discovered completely by accident during an MRI or CT scan for an unrelated issue, like a stubborn migraine or a minor concussion from a weekend soccer match. Statistics from the Brain Aneurysm Foundation indicate that roughly 1 in 50 people in the United States harbor an unruptured brain aneurysm right now. Most will live full lives without ever knowing it.
The Architecture of a Fragile Artery Wall
Where it gets tricky is understanding why these arterial blisters form in the first place. The human brain requires a massive, constant supply of oxygenated blood, which is delivered through a complex network of vessels at the base of the skull known as the Circle of Willis. Because blood flows under high pressure through these sharp bends and bifurcations, hemodynamic stress constantly batters the vessel walls. Over time, genetic predisposition, chronic hypertension, or a long history of heavy cigarette smoking can degrade the internal elastic lamina. But we're far from fully understanding the exact trigger. Why does a 4mm aneurysm stay stable for forty years in one patient, while a similar lesion in another person ruptures unexpectedly on a quiet Tuesday afternoon? Honestly, it's unclear, and anyone who claims otherwise is selling certainty where none exists.
When Size and Shape Dictate the Danger Level
Neurosurgeons do not treat every vascular anomaly they stumble across, because doing so would cause more harm than good. Instead, they obsess over morphology and dimensions. A tiny, smooth, 2-millimeter dome tucked away in a low-flow zone represents a vastly different clinical scenario than an 11-millimeter, irregular, multilobulated sac sitting directly at the basilar artery apex. I believe our current medical obsession with immediate intervention sometimes overrides patient-specific nuance, driving people toward procedures they might never actually need. Yet, we cannot simply ignore them either. The breakthrough ISUIA study (International Study of Unruptured Intracranial Aneurysms) dramatically shifted how we calculate these probabilities by showing that small lesions under 7 millimeters in the anterior circulation have an incredibly low annual rupture rate, hovering around 0.1 percent. That changes everything when you are calculating long-term survival metrics.
How Neurosurgeons Disarm the Bomb: Endovascular Coiling and Flow Diversion
The field of neurosurgery has undergone a massive paradigm shift over the last three decades, moving away from aggressive skull-opening operations toward elegant, minimally invasive, catheter-based therapies. If you had walked into a major academic medical center like the Mayo Clinic in 1995 with an unruptured aneurysm, your only real option would have been a major craniotomy. Today, interventional neuroradiologists routinely access the brain through a tiny puncture wound in the groin or the wrist, using the body's natural highway of blood vessels to fix the defect from the inside out.
The Art of Packing the Sac with Platinum
Endovascular coiling is the workhorse of modern neurovascular intervention. Under continuous fluoroscopic guidance, a specialist guides a microcatheter through the femoral artery, up through the aorta, and directly into the opening of the aneurysm sac itself. Then, they deploy microscopic, detachable platinum coils into the space. And because these wires are incredibly soft, they conform perfectly to the contours of the dome, looping around themselves like a ball of yarn until the space is entirely packed. This mesh of platinum disrupts the internal hemodynamic flow, causing the stagnant blood inside to clot and form a protective thrombus. As a result: the dangerous pressure is removed from the fragile arterial walls, effectively neutralizing the risk of a future rupture.
Flow Diversion: Redirecting the Internal Current
But what happens when the bulge is wide-necked or giant, making it impossible to keep coils safely inside the sac without them spilling out into the main artery? That is where devices like the Pipeline Embolization Device come into play, which revolutionized the industry after its initial FDA approval back in 2011. Instead of filling the actual aneurysm, the surgeon deploys a tightly woven, mesh stent across the neck of the vessel bulge. People don't think about this enough, but you are essentially rebuilding the damaged highway wall rather than patching the pothole. The dense mesh immediately diverts the main force of the blood flow away from the weakness, forcing it to continue straight down the parent artery. Deprived of its turbulent blood supply, the aneurysm gradually thromboses and shrinks over a period of months, while the body naturally grows a fresh layer of endothelial cells right over the stent scaffolding.
The Classic Alternative: Surgical Clipping Through a Craniotomy
Despite the undeniable elegance and rapid recovery times associated with endovascular techniques, traditional open brain surgery remains a foundational pillar for treating specific, complex vascular lesions. It is brutal, mechanical, and incredibly effective. If an aneurysm features an highly irregular geometry, or if it emerges at a complex arterial branch where an endovascular stent might accidentally cut off blood supply to vital surrounding brain tissue, the direct physical approach becomes the safest path forward.
The Mechanical Precision of the Titanium Clip
This procedure requires a craniotomy, meaning a neurosurgeon carefully removes a small section of the skull to create a direct window to the brain. Using an advanced operative microscope that magnifies the surgical field twenty times, they navigate the delicate corridors between the brain's lobes without disturbing the sensitive neural tissue. Once the neck of the aneurysm is fully exposed, the surgeon uses specialized apposition forceps to place a tiny, permanent titanium clip across the base. The mechanical force of the clip permanently pinches the walls together, sealing the entrance completely. Except that getting to that point requires hours of meticulous, high-stakes dissection around cranial nerves and microscopic perforating vessels where a single millimeter error can lead to a devastating stroke.
Why Open Surgery Still Wins the Longevity Battle
There is a sharp, fiercely debated divide between old-school open surgeons and the newer generation of endovascular specialists regarding long-term efficacy. While coiling lets a patient walk out of the hospital within 24 to 48 hours, those coils can sometimes settle or compact over time under the relentless pounding of the pulse, allowing blood to seep back into the dome. Surgical clipping, by contrast, offers a definitive, permanent cure with an exceptionally low recurrence rate. Once a clip is properly deployed and verified via intraoperative indocyanine green angiography, that aneurysm is dead and buried. You trade a tougher, longer recovery process upfront for the priceless psychological peace of mind that comes with knowing the problem is solved for the next thirty years.
Weighing the Options: How Doctors Select Your Path
Choosing between watchful waiting, endovascular coiling, and open surgical clipping requires a meticulous balancing act where the patient's age and overall health are weighed directly against the physical characteristics of the lesion. It is a highly collaborative decision, usually hammered out in multidisciplinary board meetings where specialists debate the merits of different approaches. The issue remains that every intervention carries a baseline risk of stroke, infection, or intraoperative rupture that must be lower than the natural risk of leaving the vessel alone.
The Critical Balance of Patient Age and Location
Consider two entirely different scenarios. A healthy 38-year-old woman discovers a 6mm aneurysm on her internal carotid artery; she has a long life expectancy, meaning her cumulative lifetime risk of a rupture is substantial. For her, proactive treatment via an endovascular approach makes immense sense. But what about an 81-year-old man with advanced heart disease who is found to have an identical 6mm lesion? His statistical life expectancy is shorter than the time it would likely take for that small, stable lesion to ever cause a problem, and the stress of anesthesia and blood thinners required for a procedure could easily trigger a fatal cardiac event. In his case, regular imaging monitoring is indisputably the wiser strategy. The math changes completely based on who is lying on the table.
Common mistakes and misconceptions about unruptured brain aneurysms
Many patients assume that discovering a bulging artery in the brain is an immediate death sentence. It is not. The problem is that the internet manufactures panic, leading people to believe every vascular anomaly requires instant, aggressive surgery. A tiny, three-millimeter aneurysm in an elderly patient carries a negligible risk of rupture, yet the psychological toll often drives unnecessary intervention. Preventative treatment is not a zero-risk gamble. Neurosurgeons must constantly balance the natural history of the lesion against the very real complications of surgery, such as ischemic strokes or arterial dissection. Because of this, watchful waiting is frequently the safest therapeutic pathway.
The "Ticking Time Bomb" illusion
Let's be clear: an unruptured aneurysm does not behave like a synchronized explosive device. Why do so many people think otherwise? It is a classic cognitive bias fueled by dramatic medical television shows. Statistics from the International Study of Unruptured Intracranial Aneurysms (ISUIA) demonstrate that small asymptomatic lesions under seven millimeters in the anterior circulation have a five-year rupture rate of nearly 0%. Except that patients rarely look at data when adrenaline takes over. They demand immediate obliteration of the sac, ignoring the fact that the diagnostic angiogram itself carries a small risk of neurological deficit.
Assuming all treatments are permanent fixes
Can doctors fix an unruptured aneurysm forever? Sometimes, they cannot. Another widespread misconception is that once a coil is deployed or a clip is applied, the issue vanishes entirely. The issue remains that tissue remodels over time. Endovascular coiling, while elegant and minimally invasive, suffers from a recurrence rate of roughly 20% to 25% due to coil compaction or neck remnants. Patients frequently miss their follow-up magnetic resonance angiograms because they assume they are cured. This oversight is dangerous. A treated aneurysm can regrow, demanding vigilant, lifelong imaging surveillance.
The critical role of PHASES score and morphology
Predicting which arterial wall will fail requires more than just measuring its diameter with a digital caliper. The PHASES score has revolutionized how neurovascular boards calculate five-year rupture risks by aggregating six distinct variables: population, hypertension, age, size, earlier subarachnoid hemorrhage, and site. Yet, numbers only tell half the story. The physical architecture of the dome—specifically the presence of daughter sacs or irregular lobes—signals extreme wall shear stress. Can doctors fix an unruptured aneurysm effectively without looking at these geometry quirks? Unlikely. A irregular five-millimeter aneurysm on the posterior communicating artery might be far more perilous than a smooth eight-millimeter sac on the internal carotid artery.
Why flow dynamics override simple geometry
We used to focus exclusively on size, which explains why older treatment guidelines look archaic today. Modern neurointervention relies heavily on computational fluid dynamics to visualize how blood swirls inside the vascular dome. High wall shear stress stagnation zones correlate heavily with localized inflammation and subsequent thinning of the tunica media. When a neuroradiologist spots these turbulent flow patterns during a dynamic angiogram, the clinical conversation shifts abruptly from conservative monitoring to active endovascular flow diversion.
Frequently Asked Questions
What is the exact success rate when doctors fix an unruptured aneurysm?
For elective endovascular procedures like coiling or flow diversion, the technical success rate hovering around occlusion exceeds 90% in modern high-volume stroke centers. The permanent neurological complication rate for these preventative interventions remains remarkably low, generally sitting between 4% and 5% across major clinical trials. Surgical clipping boasts a slightly higher definitive cure rate, but it carries a marginally elevated periprocedural morbidity risk due to the necessity of a craniotomy. Ultimately, choosing the right intervention depends heavily on the specific anatomy of the vessel neck and the overall baseline health of the patient.
Can lifestyle adjustments stop an unruptured aneurysm from growing?
You cannot change your genetic collagen composition, but you can drastically alter the hemodynamic forces tearing at your arterial walls. Absolute cessation of cigarette smoking is non-negotiable, as tobacco use accelerates matrix metalloproteinase expression, which degrades the structural integrity of the blood vessel. Rigorous blood pressure management—keeping systolic readings consistently below 130 mmHg—directly minimizes the chronic wall shear stress pushing against the weakened area. As a result: maintaining a pristine cardiovascular profile directly lowers the statistical probability of growth and subsequent catastrophic rupture over time.
How long is the recovery time after a preventative aneurysm procedure?
If you undergo an elective endovascular flow-diverter stent placement, you will typically spend just one night in the neuro-intensive care unit for close observation. Most patients return to their baseline sedentary professional activities within one to two weeks, provided their femoral or radial access site heals without hematoma formation. Open microvascular clipping demands a significantly more grueling recovery timeline, requiring a three-to-five-day hospital stay followed by four to six weeks of physical convalescence at home to allow the bone flap and temporalis muscle to heal. (And let's not forget the profound mental exhaustion that accompanies any major intracranial surgery.)
A definitive perspective on managing silent vascular risks
We must stop treating every unruptured intracranial lesion as an emergency demanding immediate mechanical obliteration. The medical community possesses highly sophisticated tools to differentiate a benign vascular asymmetry from a genuinely dangerous structural defect. Aggressive surgical intervention is a magnificent triumph of modern medicine, but deploying it indiscriminately on every microscopic sac does more harm than good. True clinical expertise lies in knowing when to wield the scalpel and when to leave the patient entirely alone. We must foster a clinical culture that prioritizes meticulous, data-driven surveillance over reactionary, fear-based operating room scheduling. In short: can doctors fix an unruptured aneurysm? Absolutely, but the real art lies in deciding whether the specific lesion actually threatens the patient's life or simply offends the radiologist's eye.