The Anatomy of Those First Sixty Seconds: What Are We Actually Measuring?
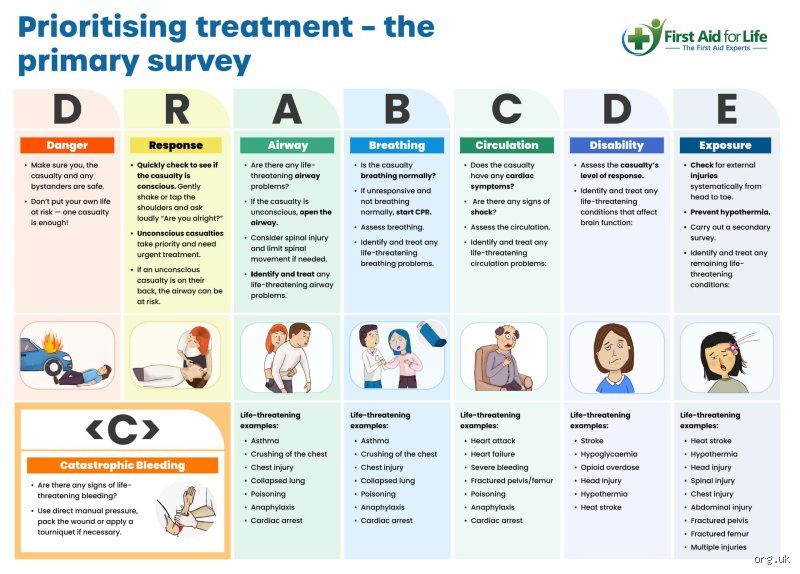
Let us look past the clean textbook scenarios for a moment. In the clinical trenches, we rely on the ABCDE protocol—Airway, Breathing, Circulation, Disability, and Exposure—to systematically prevent preventable deaths. But if you think this is a leisurely checklist, you are dead wrong.
The Illusion of the Linear Checklist
We train rookies to check the airway, then move to breathing, and then assess circulation. It looks neat on a laminated chart, except that is not how human brains process catastrophe. Experienced paramedics perform these checks simultaneously. You look at the chest rise while feeling a radial pulse and listening for stridor. It takes five seconds, not fifty. Where it gets tricky is when a practitioner gets stuck in a cognitive loop, obsessing over a complex fracture while the patient quietly suffocates from a blocked airway.
The 2024 Resuscitation Council Guidelines vs. Street Medicine
The discrepancy between institutional mandates and field reality is vast. European and American trauma guidelines updated in recent years demand an immediate catastrophic hemorrhage control phase—often called
c
ABCDE—before you even look at the mouth. If a patient is spurting blood from a femoral artery laceration, your primary assessment time for the "Airway" portion drops to zero until that bleed is stopped. I once watched a paramedic stall for two minutes trying to secure a pristine airway on a motorcycle accident victim in downtown Chicago, entirely missing the massive abdominal bruising that signaled internal bleeding. That changes everything. The textbook says under a minute, but the street says you have exactly as long as the most immediate killer allows.Deconstructing the Time Metrics Across Varied Clinical Environments
To truly understand how long should a primary assessment take, we must dissect how different environments alter our internal metronome. A brightly lit triage bay in Johns Hopkins Hospital demands a totally different cognitive speed than a muddy ditch off Route 66 at three o’clock in the morning.
The Tactical Combat Casualty Care (TCCC) Reality
In military medicine, the clock is dictated by incoming fire. Under the TCCC Care Under Fire protocols, your primary assessment might last literally three seconds. Do they have massive bleeding? Can they move? If the answer involves heavy arterial bleeding, you slap on a combat tourniquet and drag them behind cover. Here, the traditional 60-second rule is not just irrelevant—it is a death sentence for the provider.
The Wilderness Medicine Paradox
Now, flip the script completely. You are an advanced wilderness EMT on a remote ridge in the Rocky Mountains, six hours from the nearest helicopter extraction. How long should a primary assessment take here? You might spend a full 90 seconds to two minutes on the primary phase alone. Why? Because environmental exposure will kill a hypothermic patient faster than a minor internal bleed, and your physical examination must be meticulously thorough through heavy layers of technical clothing. You cannot just cut everything off with trauma shears when the ambient temperature is minus ten degrees.
Pediatric Triage and the Pediatric Assessment Triangle
Kids are not small adults, and their physiology crashes with terrifying speed. With pediatric patients, the primary assessment relies heavily on the Pediatric Assessment Triangle (PAT), which looks strictly at appearance, work of breathing, and circulation to the skin. This visual assessment takes roughly 15 seconds. It happens before you even touch the child. If a three-year-old in an urgent care clinic in Miami presents with nasal flaring and intercostal retractions, you do not need a stethoscope to know they are failing. You know within five seconds that your primary assessment has yielded an immediate red flag.
The Hidden Cognitive Friction That Slows Down First Responders
If the math is so simple, why do audits of ambulance runs show primary assessments dragging on for three, four, or even five minutes? The issue remains one of human psychology and cognitive overload.
Fixation Errors and the Siren Song of Obvious Injuries
The human brain loves a distraction. When an emergency physician encounters a patient with a compound tib-fib fracture where the bone is visibly protruding, their gaze naturally locks onto that horrific sight. But people don't think about this enough: broken legs rarely kill patients in the first five minutes. Airway obstruction does. This cognitive trap, known in medical literature as a fixation error, can inflate a primary assessment from a crisp 45 seconds to a bloated, dangerous three minutes. Experts disagree on how to train this out of people, but honestly, it's unclear if simulation training can ever truly replicate the visceral panic of real-world gore.
The Multi-Casualty Burden and Triage Tags
When a mass casualty incident occurs—like the 2013 Boston Marathon bombing—the primary assessment morphs into the START triage system (Simple Triage and Rapid Treatment). You have a maximum of 30 seconds per patient. You check respiration, perfusion, and mental status. If they aren't breathing, you open the airway once. Still nothing? You tag them black and move on. It feels cold, almost robotic, yet it is the only way to maximize survival when resources are overwhelmed. As a result: your assessment timeline drops by half because the collective good outweighs the individual.
How Expert Intuition Distorts the Standard Assessment Clock
There is a massive difference between how a novice nurse performs an assessment and how a twenty-year flight paramedic does it. It comes down to what psychologists call thin-slicing.
The "Doorway Test" and Gestalt Evaluation
Many veteran clinicians talk about the "sick or not sick" visual scan. This is not mystical intuition; it is rapid pattern recognition honed by thousands of clinical encounters. Within two seconds of walking into a resuscitation room, an experienced doctor evaluates skin pallor, posture, and conscious level. But can we trust this gut instinct? Usually, yes. Except that relying too heavily on a gestalt evaluation can cause a clinician to miss subtle signs of compensated shock, where a patient looks perfectly fine right up until their blood pressure plummets to zero. Hence, the formal ABCDE structure must still be completed, even if your gut tells you the patient is totally fine.
Algorithmic Rigidness vs. Clinical Fluidity
Medical schools love algorithms because they are easy to grade on a multiple-choice exam. But the field demands fluidity. If you are strictly counting seconds—demanding that exactly ten seconds be spent on Airway, fifteen on Breathing—you are missing the forest for the trees. A primary assessment is a dynamic loop, not a static finish line. You assess, you intervene, and you immediately reassess. If you intubate a patient, your primary assessment clock resets to zero. You are back at "A," ensuring that tube is actually in the trachea and not the esophagus, while the minutes continue to tick away outside your peripheral vision.
Common mistakes and dangerous diagnostic misconceptions
The obsession with the stopwatch
Speed kills, but paradoxically, so does sluggishness. The biggest blunder green practitioners commit is treating the clock as their primary antagonist during patient evaluation. Let's be clear: a rapid initial survey is a byproduct of clinical mastery, not a race where you trigger a timer. When you rush the airway check simply to boast a sub-fifteen-second completion, you inevitably overlook subtle tracheal deviations or muffled stridor. The problem is that frantic triage breeds cognitive blindness. You see what you expect to see, skipping the meticulous sweep of the thorax because your brain demands compliance with an arbitrary temporal benchmark.
The linear trap of rigid algorithms
Human anatomy scorns your neat checklists. Many clinicians approach the initial medical screening as a static, top-down ladder. They fixate on airway patency while the patient silently exsanguinates from a pelvic fracture hidden beneath heavy denim. Except that real-world trauma demands simultaneous, dynamic reassessment. Fixation error ruins lives. If you refuse to jump from airway to circulation out of sequence when a massive arterial spurt manifests, you are practicing dogmatic, hazardous medicine. The countdown dictates urgency, yet your clinical priority must bend to the most immediate physiological threat.
The hidden variable: Environmental cognitive load
How chaos alters your diagnostic timeline
Step outside the sterile, fluorescent comfort of an emergency department bay. How long should a primary assessment take when you are kneeling in a freezing ditch, rain pelted, with sirens screaming in your ear? The answer stretches unpredictably. Ambient noise, poor lighting, and hostile bystanders hijack your working memory, which explains why a process that takes thirty seconds in a simulation lab can easily morph into a grueling three-minute ordeal on a midnight highway. Savory expert advice dictates that you must factor in this environmental tax. Do not penalize your team for taking longer when dealing with a trapped, hypothermic patient. Instead, deliberately slow your speech down to accelerate your collective processing speed. (It sounds counterintuitive, but deliberate calmness actively suppresses the cortisol spikes that cause physical clumsiness during manual interventions.)
Frequently Asked Questions
Does a pediatric primary assessment take longer than an adult evaluation?
Yes, evaluating an infant requires an entirely different temporal budget due to anatomical fragility and communication barriers. Statistics from pediatric emergency networks indicate that up to forty percent of initial infant assessments require an additional forty-five seconds just to establish an accurate baseline respiratory rate without agitating the patient. You cannot simply rush a toddler with a stethoscope without triggering a crying fit that masks critical breath sounds. As a result: the timeline expands because you must rely heavily on the Pediatric Assessment Triangle before you even touch the skin. This observational phase consumes precious ticks but prevents the diagnostic errors common in chaotic pediatric codes.
How does the introduction of telemedicine impact the initial patient evaluation?
Remote oversight drastically alters how long should a primary assessment take because it introduces a digital screen between the specialist and the physical body. Data from rural trauma networks reveals that camera positioning, audio lag, and relaying commands to on-site technicians adds an average of sixty-two seconds to the overall diagnostic sequence. But is this delay automatically detrimental to the human on the stretcher? Not necessarily, because the remote eyes frequently catch subtle neurological deficits or pupil asymmetries that a frantic, hands-on paramedic might miss in the heat of the moment. The issue remains one of balancing technological latency against the undeniable benefit of immediate, real-time board-certified expertise.
Should you halt the assessment if you discover an immediate life threat?
Absolutely, because the entire philosophy of this rapid initial survey hinges on the strict rule of fix-as-you-find. You never proceed to checking disability or exposure if the patient has a completely obstructed airway or a massive, catastrophic external hemorrhage. Internal clinical audits show that failing to stop and address an occluded airway immediately increases mortality by fourteen percent per minute of delayed intervention. In short, the clock stops for no one, but your progression through the mnemonic must freeze until oxygenation and basic perfusion are secured.
The definitive stance on diagnostic velocity
Stop looking for a universal, magic number because a rigid temporal benchmark is a dangerous fiction fabricated by bureaucrats who have never wiped blood off their own boots. The duration of your initial medical screening must remain elastic, governed entirely by the shifting physiology of the human suffering right in front of you. We must cultivate a culture that prioritizes clinical thoroughness over reckless speed, demanding that practitioners master the art of deliberate, aggressive precision. If you are cutting corners just to hit a mythical sixty-second metric, you are failing your patient and violating your oath. True mastery means knowing exactly when to move like lightning and when to pause, breathe, and re-evaluate the entire clinical picture.