The Anatomy of a Silent Bulge: What Are Brain Aneurysms Doing to Our Statistics?
We need to talk about what we are actually measuring here. A cerebral aneurysm is essentially a blister on a blood vessel, a weakened spot in the arterial wall that balloons outward under the constant thumping of cardiac pressure. Most people live their entire lives with these tiny outpouchings, completely oblivious to their existence, until an unrelated migraine or a minor concussion lands them in an emergency room for an MRI. That changes everything for the statistics. Suddenly, an incidental finding becomes a data point, inflating the perceived prevalence of what was once considered a rare affliction.
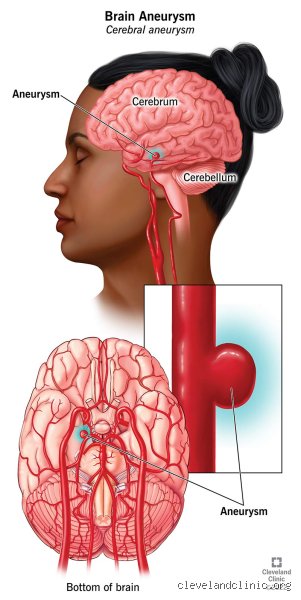
The Circle of Willis and the Geography of Weakness
Where it gets tricky is the specific architecture of our cerebral plumbing. The brain relies on a beautiful, redundant ring of arteries at its base called the Circle of Willis, and this is exactly where the vast majority of intracranial aneurysms choose to form. Why? Because the physics of fluid dynamics at these arterial junctions are brutal. Blood doesn't just flow smoothly; it slams into these forks like a rushing river hitting a fork in the canyon. If you have an inherited weakness in the internal elastic lamina—the structural scaffolding of the artery—a bulge is almost inevitable over decades of pumping. But honestly, it's unclear why some people with textbook-perfect vasculature develop them while others with rampant risk factors remain completely clear.
Counting the Unseen: How Common Are Brain Aneurysms Across Diverse Populations?
Let's look at the raw numbers because the epidemiological data paints a fascinating, if occasionally contradictory, picture. For decades, the gold standard estimate has hovered around 2% to 3% of the general population, a figure derived from massive autopsy studies and retrospective reviews of angiograms. But we're far from a uniform distribution across the globe. If you look at retrospective data from places like the Mayo Clinic in Rochester, Minnesota, or neurological registries in Helsinki, Finland, the numbers twist sideways. Finland and Japan, for reasons that still provoke fierce arguments among geneticists, exhibit significantly higher rates of both prevalence and subarachnoid hemorrhage than Western Europe or North America.
The Skewed Reality of Autopsy Data versus Modern Neuroimaging
And this is where our historical understanding of how common are brain aneurysms starts to fracture under modern scrutiny. Early 20th-century autopsy protocols were notoriously variable; a pathologist in 1950 might meticulously dissect the basilar artery while another might gloss over a tiny two-millimeter sac on the anterior communicating artery. Today, high-resolution CT angiography can detect abnormalities smaller than a grain of rice, which explains why contemporary screening studies sometimes push the estimated prevalence closer to 5% in specific older demographics. I strongly believe we are over-diagnosing the significance of these tiny lesions while simultaneously underestimating the systemic vascular weaknesses that cause them in the first place.
Age, Gender, and the Hormonal Cliff
The demographic split is unequal. Brain aneurysms are distinctly rare in children, but the curve steepens dramatically once people hit their fourth and fifth decades of life. Women are disproportionately affected, outnumbering men by a ratio of roughly 3 to 2. The issue remains: why does this gender disparity widen so aggressively after menopause? The prevailing medical consensus points toward the protective qualities of estrogen, which helps maintain the structural integrity of endothelial cells. When that hormonal shield drops during the late forties, the arterial walls in the brain seem to lose their resilience, making women in this age bracket the primary demographic for newly discovered unruptured aneurysms.
The Catalyst of Risk: What Actually Drives the Prevalence Higher?
People don't think about this enough, but a brain aneurysm is rarely a solo act of bad luck; it is usually the product of a long, toxic relationship between genetic predisposition and environmental insults. You can't change your family tree, but you can certainly change how hard your blood slams against your arterial walls every second of the day.
The Lethal Synergy of Nicotine and Hypertension
Smoking is the absolute king of acquired risk factors, increasing the likelihood of aneurysm formation by a factor of nearly four. It isn't just about localized inflammation; the chemicals in tobacco smoke actively degrade the collagen matrix within the vessel walls, rendering them brittle. Pair a 20-pack-a-year smoking habit with chronic, untreated essential hypertension, and you have created the perfect hydrodynamic storm. The constant, elevated hydrostatic pressure chips away at the weakened vessel, inflating the aneurysm like a cheap balloon. Yet, despite this well-documented mechanism, millions of hypertensive smokers will never develop a single vascular bulge, a nuance that defies the simplistic scare tactics often found in public health pamphlets.
Inherited Connective Tissue Disorders: The Genetic Blueprint
For a small segment of the population, the deck is stacked from birth. Individuals diagnosed with Autosomal Dominant Polycystic Kidney Disease (ADPKD) or vascular Ehlers-Danlos syndrome live with a fundamentally flawed blueprint for cellular matrix construction. If you have ADPKD, the prevalence rate jumps from the standard 2% up to an alarming 10% or even 20%. For these families, screening isn't an academic question; it is a clinical necessity because the structural integrity of their entire circulatory system is compromised from the outset.
Sifting Through the Noise: Rupture Rates versus Incidental Prevalence
To truly understand how common are brain aneurysms, we must aggressively decouple the presence of an aneurysm from its rupture. They are entirely different clinical beasts. The public hears the word "aneurysm" and immediately visualizes a catastrophic, life-ending bleed, but the data tells a vastly more comforting story about stability.
The International Study of Unruptured Intracranial Aneurysms (ISUIA) Benchmark
The landmark ISUIA study, which tracked thousands of patients across dozens of centers globally, sent shockwaves through the neurosurgical community by demonstrating that small aneurysms—those measuring less than 7 millimeters in diameter on the anterior circulation—have an annual rupture rate of virtually 0% in patients with no prior history of hemorrhage. Think about that for a second. A tiny bubble in the front of the brain is statistically safer to leave alone than to operate on, given the inherent risks of open craniotomy or endovascular coiling. It turns out that the vast majority of these vascular anomalies are completely stable, benign tenants in the cranium, resembling slow-moving geological formations rather than active volcanoes.
The Critical Cut-Off: When Size and Location Dictate Danger
But when an aneurysm creeps past that 7-millimeter threshold, or if it is located in the posterior circulation—such as the basilar or vertebral arteries—the math changes instantly. A 12-millimeter aneurysm resting on the posterior communicating artery carries a profoundly different prognosis, where the annual risk of a catastrophic subarachnoid hemorrhage can climb past 1% to 2% per year. Over a decade, that cumulative risk becomes unacceptable. Hence, specialists must balance the structural mechanics of the lesion against the patient's life expectancy, an exercise in clinical gambling that relies as much on intuitive experience as it does on rigid statistical tables.
Common mistakes and public misconceptions
The "ticking time bomb" fallacy
We need to dismantle the pervasive myth that every unruptured intracranial aneurysm is a lethal countdown timer. People discover an incidental finding on an MRI and immediately draft their wills, paralyzed by sheer terror. But let's be clear: the vast majority of these vascular bulges never burst. Medical literature indicates that roughly 50 to 80 percent of all aneurysms remain completely asymptomatic throughout a person's lifespan. Why do we assume every weak spot in an artery wall equals an impending catastrophe? The answer lies in dramatic medical television, which routinely ignores the boring reality of stable, calcified vascular walls.
Equating size directly with guaranteed rupture
Another frequent blunder involves obsessing exclusively over diameter. Except that biology despises simple, linear rules. You might assume a 3mm bulge is inherently safe while a 12mm lesion is a guaranteed disaster. The issue remains that morphology, location, and hemodynamic stress dictate behavior far more than a single millimeter measurement. An irregular, lobulated 4mm anterior communicating artery aneurysm can possess a significantly higher rupture propensity than a perfectly smooth 8mm internal carotid lesion. Neurosurgeons do not just pull out a ruler; we evaluate the architectural geometry of the entire circle of Willis.
Misunderstanding the true genetic link
Because a distant aunt suffered a subarachnoid hemorrhage, you might convince yourself that your neurological destiny is already sealed. Yet, isolated familial instances rarely justify widespread panic. True hereditary risk clusters within specific parameters, namely having two or more first-degree relatives diagnosed with a brain aneurysm. If you only have one vague second-degree relative with a history of hemorrhagic stroke, your baseline probability barely nudges above the general population average of one in fifty.
The hemodynamic microenvironment: Expert advice on hidden triggers
Why wall shear stress beats simple blood pressure
Standard clinical counsel always emphasizes managing systemic hypertension, which makes perfect sense on paper. But what if we are looking at the wrong mechanical force? The problem is that systemic blood pressure is merely a global metric, whereas wall shear stress and localized turbulent flow drive the actual degradation of the internal elastic lamina. Think of it like a river bending violently around a sharp cliff; the outer curve erodes exponentially faster due to fluid dynamics, regardless of whether the river is experiencing a flood or a normal current. As a result: an individual with pristine, athletic blood pressure can still experience lesion growth if their unique vascular anatomy creates a localized vortex.
My definitive advice to patients who discover an unruptured lesion is to abandon the frantic, counterproductive elimination of all physical exertion. Do not stop lifting groceries or enjoying moderate cardiovascular exercise out of fear. Instead, ruthlessly eliminate chronic nicotine exposure and sustained, unmanaged stress spikes, as these specific factors actively alter the biological endothelium, making the vessel walls brittle. We cannot easily remodel your genetic arterial geometry, but we can absolutely prevent you from chemically accelerating its decay.
Frequently Asked Questions
What are the actual statistical odds of a brain aneurysm rupturing out of nowhere?
The annual rupture rate for a typical, small unruptured intracranial lesion hovering under seven millimeters is surprisingly low, generally estimated at less than 1 percent per year. When you track that data across a decade, the cumulative risk sits at roughly 5 to 10 percent, depending heavily on whether the patient actively smokes or possesses a history of previous subarachnoid hemorrhages. Which explains why watchful waiting via serial magnetic resonance angiograms is frequently the safest, most logical clinical pathway. Do you really want to undergo invasive prophylactic endovascular coiling or an open craniotomy for a lesion that has a 99 percent chance of doing absolutely nothing this year? We must balance the concrete 2 to 3 percent risk of surgical complications against the microscopic annual probability of a spontaneous bleed.
Can lifestyle modifications actively shrink an existing vascular bulge?
Once the structural matrix of the arterial wall has degraded enough to create an outpouching, the anatomical change is permanent and cannot be reversed through diet, supplements, or holistic therapies. Tobacco cessation and meticulous blood pressure regulation are paramount for preventing further enlargement, but they will not miraculously restore the vessel to its original, linear shape. It is a one-way structural degradation, much like a balloon that has been overinflated and then partially deflated, leaving the rubber permanently stretched and thinned. Therefore, the goal of conservative management is absolute stabilization rather than lesion regression.
How common are brain aneurysms in children compared to the adult demographic?
Pediatric intracranial lesions are exceedingly rare anomalies, accounting for less than 2 percent of all documented cases worldwide. Unlike adult lesions which stem from decades of hemodynamic wear and tear, childhood cases typically arise from severe head trauma, systemic infections, or congenital connective tissue disorders like Ehlers-Danlos syndrome. They also exhibit a strange, unexplained male predominance, contrasting sharply with the adult population where women are twice as likely to develop a vascular bulge. (Interestingly, pediatric variants also tend to be much larger and more complex, frequently classified as giant lesions exceeding twenty-five millimeters).
A definitive paradigm shift in vascular awareness
We must stop treating the incidental discovery of a brain aneurysm as an immediate death sentence and start viewing it as a manageable, chronic vascular trait. The medical establishment routinely traumatizes patients with aggressive, unnecessary interventions driven more by medicolegal anxiety than actual clinical data. Finding a bulge on a scan is an opportunity for targeted lifestyle modification, not an eviction notice from life. We need to cultivate a clinical culture that respects the resilience of human vasculature while remaining vigilant. Let us replace blind panic with sophisticated, individualized hemodynamic monitoring. Your biology is not a fragile ticking clock; it is a complex, adaptive system that frequently thrives despite structural imperfections.