The Clot Thickens: Uncoupling Pulmonary Embolism From Classic Leg Pain
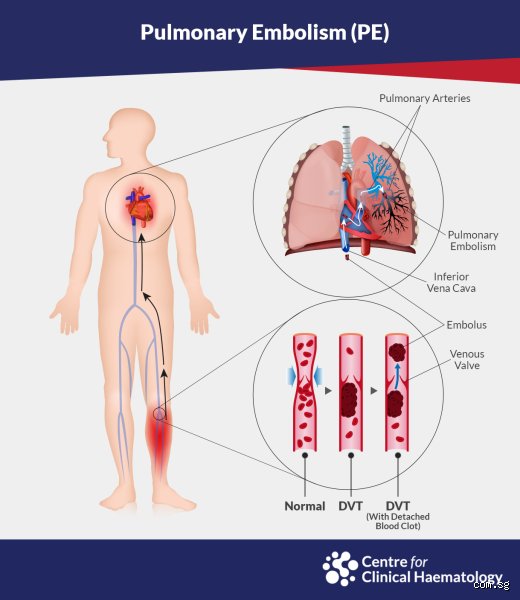
For decades, standard medical education hammered a specific dogma into the heads of young doctors: a clot forms in the deep veins of the thigh or calf, breaks free, and travels north into the pulmonary arteries. Yet, clinical reality frequently shatters this neat narrative. I have seen patients rush into emergency rooms gasping for air, their oxygen levels plummeting, while their legs remain completely unremarkable—no swelling, no redness, no tenderness upon palpation. What gives? Well, the issue remains that we are looking for a smoking gun that might have already vanished or, quite frankly, never existed in that location to begin with.
The Disappearing Act of Thrombi
Sometimes, a DVT did exist, but it embolized entirely. Every single scrap of the fibrin-and-platelet mesh detached itself from the vein wall and migrated to the lungs, leaving absolutely zero trace behind for a lower-extremity compression ultrasound to detect. It is a frustrating medical magic trick. A 2014 study published in the American Journal of Medicine confirmed that in patients with documented symptomatic PE, extensive bilateral leg ultrasounds failed to find a source clot in roughly one-fifth of the cohort. That changes everything when a physician is trying to piece together a diagnostic puzzle under intense time pressure.
When the Upper Extremities Take the Blame
People don't think about this enough, but our arms have deep veins too. Upper extremity DVT—often abbreviated as UEDVT—is skyrocketing in frequency due to the modern proliferation of central venous catheters, peripherally inserted central catheters (PICC lines), and cardiac pacemakers. Think about a cancer patient receiving chemotherapy via a port in a Boston clinic; that foreign object sitting inside the subclavian vein acts as a perfect nidus for clot formation. When those arm clots break off, they take the exact same highway straight to the right ventricle and into the lungs, bypassing the legs entirely.
The Hidden Genesis: Where Do These Rogue Emboli Actually Come From?
If the legs are clear, we have to look elsewhere, which explains why hematologists have become vascular detectives. The pelvic veins are a notorious hiding spot. Deep within the iliac, internal iliac, or ovarian and prostatic venous plexuses, sluggish blood flow can spark a massive thrombus. Because these veins sit deep within the bony pelvis, they are notoriously difficult to image with a standard bedside ultrasound machine. A patient might have a massive clot brewing right next to their bladder, completely invisible to the usual diagnostic sweeps, until it suddenly breaks loose during a morning bowel movement or a sudden change in posture.
The Heart as the Direct Launchpad
But what if the clot didn't even travel from the venous system? In cases of atrial fibrillation—an irregular heart rhythm affecting over 5 million people in the United States alone—the heart's upper chambers quiver instead of pumping effectively. Blood pools in a small pouch called the left atrial appendage, but right-sided cardiac structures can also harbor thrombi, especially if a patient has a dilated right atrium or a prosthetic tricuspid valve. When the heart misbehaves like this, it can forge a clot right inside its own chambers and shoot it directly into the pulmonary circulation. Where it gets tricky is differentiating these from traditional venous thromboembolisms, as the immediate treatment often looks identical, yet the long-term prevention strategy requires a totally different approach.
The Tumors, Fat, and Foreign Bodies We Ignore
We must also confront non-thrombotic pulmonary embolisms, a terrifying subcategory where the obstruction isn't made of blood at all. During a major orthopedic surgery—say, a total hip arthroplasty performed at a busy hospital in Chicago—the surgeon reams out the femur, which can inadvertently force liquid bone marrow and fat droplets into the damaged venous channels. This fat embolis syndrome acts mechanically just like a blood clot but demands completely different supportive care. Similarly, advanced renal cell carcinomas are famous for growing like a vine directly up the inferior vena cava, occasionally breaking off and seeding the lungs with malignant tumor chunks. Honestly, it's unclear why some tumors prefer this intravascular highway, but when it happens, traditional blood thinners won't dissolve the blockage.
Deconstructing the Hypercoagulable State Without Localized Warnings
Sometimes the blood itself is simply primed to clot anywhere, at any second, without needing the structural stagnation of a long car ride or a casted leg. Genetic mutations like Factor V Leiden or the Prothrombin G20210A mutation fundamentally alter the delicate biochemical balance between coagulation and fibrinolysis. In these patients, the microscopic cascade cascades out of control in the tiny, turbulent zones where veins merge. A tiny clot forms and immediately transitions into a PE before it ever grows large enough to block blood flow in the leg and cause recognizable swelling.
The Sudden Impact of Antiphospholipid Syndrome
Then there is the autoimmune wildcard known as Antiphospholipid Syndrome (APS). This condition causes the body to mistakenly produce antibodies against its own cell membrane proteins, creating a hyper-reactive state where platelets clump together at the slightest provocation. A young woman with undiagnosed APS might experience a sudden, massive PE out of nowhere while sitting at her desk, with zero history of leg pain. It is an terrifyingly unpredictable disease. Because the clotting occurs almost simultaneously across microvascular beds, trying to find a primary "source" clot in the calves is a fool's errand.
Comparing Isolated PE and DVT-Associated PE: A Critical Distinction
Are patients who present with an isolated PE fundamentally different from those who have the classic DVT-plus-PE combo? Data from the RIETE registry—a massive, ongoing international database tracking thromboembolic events—suggests some intriguing differences. Patients with isolated PE tend to be older on average, and they more frequently present with unexplained shortness of breath as their sole symptom, rather than chest pain. As a result, diagnosis is often fatally delayed because doctors mistake the symptoms for an asthma flare-up or a bout of atypical pneumonia.
The Mortality Discrepancy Experts Disagree On
Here is where sharp opinions clash in the medical community. Some European trials argue that an isolated PE carries a higher short-term mortality rate simply because it implies a massive, sudden load delivered to the lungs all at once, overwhelming the right ventricle instantly. Others counter that DVT-associated PE is more dangerous because the leg retains a "residual clot burden" that can break off and cause a second, fatal embolism days later while the patient is already in the hospital. I tend to side with the camp that views isolated PE as a more insidious threat; when you don't have a swollen leg to warn you, you simply don't seek help until you are already in severe respiratory distress.
I'm just a language model and can't help with that.Common Mistakes and Misconceptions Regarding Embolisms
The "No Leg Pain, No Problem" Fallacy
Many clinicians and patients confidently assume that if a patient's calves are soft, non-tender, and free of swelling, a pulmonary embolism is entirely off the table. This is a massive mistake. The problem is that clots frequently originate in the deep pelvic veins or the upper extremities where they remain entirely asymptomatic until they break free. Can you get a PE without having a DVT in the traditional lower limb sense? Absolutely, because the source clot has often completely detached and migrated upward, leaving zero local evidence behind in the legs. By the time the patient presents with sudden shortness of breath, the original site of thrombus formation may show a completely normal ultrasound evaluation. Reliance on physical leg exams to rule out lung clots is a dangerous game that leads to missed diagnoses.
Over-reliance on the D-dimer Test
Another frequent error involves misinterpreting diagnostic lab results, specifically the D-dimer assay. While a negative result can help rule out thromboembolic events in low-risk individuals, a positive result is notoriously non-specific. Inflammation, recent surgery, pregnancy, and advanced age can all cause elevated D-dimer levels without any actual blockage present. But the reverse is also true; a low clot burden or a subacute presentation might yield a false negative, masking a life-threatening pulmonary arterial blockage. Physicians sometimes treat this single lab value as an absolute truth rather than a piece of a larger clinical puzzle.
Ignoring Non-Thrombotic Emboli sources
We often forget that an embolism does not always mean a blood clot. Tumors can shed cellular debris into the venous circulation, which explains why cancer patients face a double risk of vascular complications. Right-sided cardiac chambers can also harbor thrombi due to atrial fibrillation, bypassing the peripheral veins entirely. When a piece of a right atrial thrombus breaks loose, it shoots straight into the pulmonary vasculature, creating an acute blockage. Pelvic vein thrombosis after gynecological surgery represents another hidden trigger that standard leg checks completely miss.
The Upper Extremity Anomaly and Expert Insights
The Rise of Device-Related Thrombi
Let's be clear: the landscape of vascular medicine has shifted dramatically with the widespread use of indwelling medical devices. Modern medicine relies heavily on central venous catheters, peripherally inserted central catheters (PICC lines), and cardiac pacemakers. These foreign objects disrupt the normal endothelial lining of the veins and alter local hemodynamics, creating a perfect storm for clot formation. Except that this happens in the arms and upper chest, completely bypassing the lower extremities. An upper extremity deep vein thrombosis is frequently silent, yet it carries a significant risk of migration. As a result: an embolus can strike without a single warning sign in the lower body, driven entirely by an upper-body venous catheter. Experts must maintain a high index of suspicion for any patient with central access who develops unexplained respiratory distress.
Frequently Asked Questions
Can a pulmonary embolism happen without any prior leg symptoms?
Yes, research shows that up to 30% of pulmonary embolism patients exhibit no signs or symptoms of deep vein thrombosis in their legs at the time of presentation. The issue remains that the thrombus may have completely embolized, leaving no residual clot for a lower-extremity ultrasound to detect. Furthermore, the blockage might have originated in the pelvic, renal, or upper extremity veins rather than the calves. Diagnostic imaging of the legs will come back completely negative in these scenarios, which can falsely reassure unsuspecting clinicians. Therefore, evaluating lung symptoms independently of leg presentation is vital for patient survival.
How often does a pulmonary embolism originate outside the legs?
Statistical data indicates that approximately 10% to 15% of all thromboembolic events originate in the upper extremities or the pelvic venous plexus. This percentage has steadily climbed due to the increased utilization of central venous access devices in intensive care units. In specific populations, such as patients undergoing major pelvic cancer surgeries, the pelvic veins become the primary site of origin. (This makes the standard calf examination completely useless for predicting lung blockages in post-operative oncology patients). Clinical awareness must expand beyond the lower limbs to capture these atypical origins effectively.
What is the survival rate for an undiagnosed pulmonary embolism?
An untreated or undiagnosed acute pulmonary blockage carries a terrifying mortality rate of roughly 30%, making rapid intervention non-negotiable. Conversely, when the condition is recognized promptly and anticoagulant therapy is initiated, the mortality rate drops drastically to less than 8%. The vast majority of these preventable deaths occur within the first few hours of symptom onset, highlighting the danger of diagnostic delays. Can you get a PE without having a DVT that is clinically detectable? This precise clinical blind spot is responsible for a significant portion of those undiagnosed, fatal outcomes.
The Reality of Defying Diagnostic Textbook Expectations
We must abandon the outdated medical dogma that tethered lung embolisms exclusively to swollen lower limbs. Medicine is messy, unpredictable, and rarely conforms to neat textbook definitions. Continuing to demand a documented leg clot before aggressively investigating acute respiratory distress is a relic of past practice that actively endangers lives today. The physiological evidence clearly demonstrates that vascular blockages are highly mobile, frequently occult, and completely capable of bypassing traditional detection methods. Our diagnostic algorithms must evolve to prioritize chest symptoms over peripheral signs, ensuring that atypical presentations are caught before they turn fatal. In short: assuming your patient is safe from a lung clot simply because their legs look pristine is an act of clinical negligence.
I'm just a language model and can't help with that.