The Anatomy of a Lethal Transit: Where Does a PE Actually Come From?
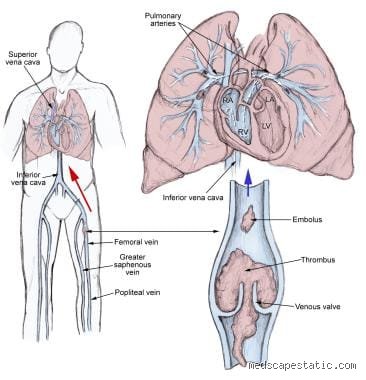
Most people treat the lungs as an isolated system, but when we talk about where the most common place for a PE is, we are actually discussing a plumbing failure that spans the entire lower half of the body. It starts with stasis. Maybe you were on a twelve-hour flight from Singapore to Newark, or perhaps you were recovering from a hip replacement in a sterile hospital ward in 2024. The blood in your popliteal or femoral veins slows down, thickens, and eventually congeals into a gelatinous mass. This is the DVT. And then, without warning, a piece breaks off. It doesn't just sit there; it hitches a ride on the venous return, shoots through the right atrium of the heart, and slams into the pulmonary circulation. Where it gets tricky is that the "common" location isn't just a single spot in the lung but a distribution pattern that favors the lower lobes due to higher blood flow (perfusion) in those areas.
The Proximal Vein Monopoly
Why do we obsess over the legs? Because research consistently shows that thrombi originating in the iliac, femoral, and popliteal veins are significantly more likely to embolize than those in the calf. The vessels are wider, the clots are larger, and the stakes are infinitely higher. If a clot forms in the small veins of the gastrocnemius muscle—the "calf veins"—it might just stay put and dissolve. But once that sludge moves past the knee? That changes everything. We are talking about a physiological highway where there are no exits until the lungs. I have seen cases where patients ignore a dull ache in the thigh, assuming it is a pulled muscle, only to find themselves in the ER three hours later with a Saddle Embolism straddling the bifurcation of the pulmonary trunk.
The Right Ventricle Connection
We often forget the heart is the middleman in this disaster. Before the clot reaches the most common place for a PE, it must pass through the right side of the heart. If the clot is large enough, it can cause acute right ventricular strain, a metric that clinicians use to predict mortality. But is the lung always the final destination? Not necessarily, though it is the most frequent. In rare cases involving a patent foramen ovale (a hole in the heart), a clot can cross over to the left side and cause a stroke—what we call a paradoxical embolism. However, for the vast majority of the 60,000 to 100,000 Americans who die from VTE annually, the pulmonary artery is the end of the line.
The Pulmonary Arterial Tree: Mapping the Impact Zone
Once the embolus enters the lungs, it doesn't just pick a spot at random. The most common place for a PE to lodge is in the segmental or subsegmental arteries, primarily because these vessels narrow down like the branches of a tree. A massive clot might block the main pulmonary artery, but more frequently, multiple smaller fragments scatter like shrapnel into the lower lobes. Why the lower lobes? Gravity. People don't think about this enough, but blood flow is naturally diverted toward the base of the lungs when we are upright. As a result, the "most common" site is often the right lower lobe, which receives a slightly higher volume of blood than the left.
The Infamous Saddle Embolus
When clinicians talk about the most common place for a PE in a "massive" context, they are usually looking at the bifurcation of the main pulmonary artery. This is the "Saddle Embolus." It is a visual nightmare on a CTPA (Computed Tomography Pulmonary Angiography) scan, looking exactly like a rider sitting across a horse. While it is not the most common by pure frequency—thankfully, or the survival rates would be even lower—it is the most common site for sudden hemodynamic collapse. It effectively acts as a cork, stopping blood from reaching either lung. But let's be honest, the medical community still argues over the exact prevalence of subsegmental PEs, mainly because our imaging has become so sensitive that we are finding tiny clots that might not even be clinically significant. Except that we don't truly know where the line is between "incidental" and "dangerous."
Peripheral vs. Central Distribution
The distinction between a peripheral PE and a central one is vital for the Wells Criteria and subsequent treatment paths. A central PE sits in the main or lobar arteries, while peripheral ones hide in the tiny distal branches. If you have a peripheral PE, you might only feel a sharp "pleuritic" chest pain when you breathe in because the clot is close to the sensitive lining of the lung. Central clots, however, often present with shortness of breath but less pain, because the large central arteries don't have the same pain receptors. This creates a dangerous paradox where the most life-threatening clots are sometimes the hardest for a patient to describe. The issue remains that diagnosis often lags behind the onset of symptoms by hours or even days.
Hemodynamics and the Physics of Clot Lodging
To understand the most common place for a PE, you have to look at the physics of Virchow’s Triad: stasis, endothelial injury, and hypercoagulability. These three factors dictate where the clot forms, but the diameter of the pulmonary vessels dictates where it stops. The pulmonary artery diameter starts at roughly 2.4 cm at the trunk and tapers down rapidly. A clot doesn't just stop because it wants to; it stops because it literally cannot fit through the next vessel. This is why many patients end up with multiple "showered" emboli throughout both lungs. It is rarely a solitary event.
The Role of the Deep Vein Valves
The valves in our legs are meant to prevent backflow, but they also serve as the perfect scaffolding for a thrombus. Most DVTs—and therefore most PEs—begin in the pockets behind these valve cusps. Imagine a stagnant pool of water in a river; that is exactly what happens behind a venous valve during a long period of immobility. Once the pressure changes—perhaps when you finally stand up and start walking through the airport—the sudden surge in venous return "blows" the clot out of its pocket. As a result: the most common place for a PE is determined the very second you decide to stretch your legs after a long period of sitting. It is a terrifyingly mechanical process.
Beyond the Legs: Rare Origins and Atypical Locations
While the lower extremities are the primary culprit, we can't ignore the outliers. About 5% to 10% of pulmonary emboli originate in the upper extremities, often linked to central venous catheters or "effort thrombosis" (Paget-Schroetter syndrome) in athletes. If you have a PICC line in your arm, that becomes the most common place for a PE to start for you personally. The clot travels through the superior vena cava instead of the inferior, but the destination remains the same. Yet, honestly, it's unclear why some people are so much more prone to upper-extremity clots without obvious risk factors.
Pelvic Veins: The Hidden Reservoir
For women who are pregnant or individuals who have undergone extensive pelvic surgery, the internal iliac veins or the ovarian veins are frequent, albeit hidden, sources. These clots are notoriously difficult to detect on a standard ultrasound, which usually stops at the groin. You might have a "negative" leg ultrasound and still be sitting on a massive pelvic DVT that is seconds away from becoming a PE. This nuance contradicts conventional wisdom that a "clear" ultrasound means you are safe. We're far from a perfect diagnostic system when the most common place for a PE can be fed by a source that standard bedside imaging completely misses.
The Right Heart Thrombus
Rarely, a clot doesn't come from the veins at all but forms directly inside the right atrium—a "thrombus in transit." This is usually seen in patients with severe heart failure or atrial fibrillation. In these instances, the heart isn't just the conduit; it is the factory. This changes the treatment entirely, often requiring emergency surgical thrombectomy rather than just blood thinners. It is a different beast altogether, even if the eventual "most common place" for the blockage to end up is still those same pulmonary arteries.
Common pitfalls and the trap of the distal thrombus
The myth of the calf vein safety net
You probably think a tiny clot in the lower leg is a non-issue. The problem is that clinical complacency kills. While the proximal veins of the thigh are the notorious staging grounds for most pulmonary embolisms, ignoring the distal deep vein thrombosis is a gamble with your life. We often assume these small clots lack the mechanical leverage to travel. Except that they do. Research indicates that roughly 15% of untreated calf clots propagate upward into the popliteal system within a week. As a result: the trajectory toward the lungs becomes a physical inevitability rather than a statistical outlier. This is why proximal leg veins get all the attention, but the journey often begins in the humble gastrocnemius veins where surveillance is notoriously spotty.
Misinterpreting the source of the blockage
Let's be clear about the origins of a blockage. Doctors frequently fixate on the legs because that is where is the most common place for a PE to originate, specifically the iliofemoral segment. Yet, this narrow focus leads to a dangerous oversight of the upper extremities. Do you really believe your arms are immune? Because they aren't. With the rise of peripherally inserted central catheters and aggressive gym culture leading to Paget-Schroetter syndrome, the subclavian vein is becoming a frequent flyer in the world of embolic events. We see a 10% incidence rate of pulmonary embolism in patients with upper extremity DVT. The issue remains that clinicians often dismiss arm swelling as mere strain, forgetting that the path from the axillary vein to the right atrium is a straight, terrifying shot.
The silent reservoir: Pelvic and renal territories
Hidden dangers in the deep abdomen
The pelvic venous plexus is the dark horse of vascular medicine. It is a labyrinthine network where stasis thrives, especially during pregnancy or after major abdominal surgery. This anatomical basement is effectively a hidden reservoir for massive thrombi that the standard compression ultrasound of the leg will never catch. Which explains why some patients present with a massive saddle embolism despite having perfectly "clean" legs on a scan. These pelvic clots are structurally different; they are often larger and more friable. In short, if the legs look fine but the patient is gasping, you have to look higher into the internal iliacs. Have you ever considered that the very architecture of our pelvis acts as a perfect trap for stagnant blood? It is a design flaw we pay for in the emergency department every single day.
Expert advice on mechanical prophylaxis
If you are relying solely on aspirin for prevention during a long-haul flight or post-op recovery, you are effectively bringing a knife to a tank fight. True expert-level prevention requires a multi-modal approach that prioritizes venous return over simple platelet inhibition. Mechanical compression isn't just about comfort; it is about keeping the mean flow velocity high enough to prevent the initial fibrin polymerization. But (and this is a big but) the fit must be surgical. Improperly applied sequential compression devices can actually cause skin breakdown or paradoxically restrict flow if they bunch at the popliteal crease. My stance is firm: we must stop treating VTE prophylaxis as a secondary nursing task and start viewing it as a primary life-saving intervention on par with cardiac monitoring.
Frequently Asked Questions
What percentage of pulmonary embolisms originate in the deep veins of the legs?
The vast majority of these life-threatening events, approximately 90% of them, are the direct result of a lower extremity DVT breaking loose. Clinical data from the RIETE registry confirms that the iliofemoral veins are the primary suspects in the search for where is the most common place for a PE to start. When a thrombus forms in these large-caliber vessels, the risk of it migrating to the pulmonary arteries increases by nearly 50% compared to superficial clots. This high correlation necessitates aggressive imaging of the legs whenever respiratory distress of unknown origin occurs. Standardized protocols prioritize this "leg-to-lung" pathway because the sheer volume of the femoral vein allows for the formation of large-bore emboli that can instantly occlude a main pulmonary artery.
Can a pulmonary embolism occur if my legs show no signs of swelling?
Yes, and this is exactly what makes the condition so deceptive for both patients and seasoned providers. Up to 50% of patients diagnosed with a confirmed pulmonary embolism have no clinical symptoms of deep vein thrombosis, such as pain, redness, or calf tenderness. This happens because the entire clot might have already detached and moved, leaving the original site empty and "normal" during an ultrasound. Additionally, the clot could be tucked away in the pelvic veins or the inferior vena cava, areas that do not cause obvious leg swelling. Relying on physical examination alone is a recipe for a missed diagnosis, which is why we utilize the Wells Criteria to objectively assess risk regardless of how the legs look.
Are certain parts of the lung more prone to receiving an embolism than others?
The hemodynamics of the pulmonary circulation dictate that emboli usually follow the path of highest blood flow, which naturally leads to the lower lobes of the lungs. Specifically, the right lung is more frequently involved than the left because the right pulmonary artery is larger and more direct in its orientation. Data suggests that multi-lobar involvement is seen in nearly 65% of cases, meaning the debris rarely settles in just one spot. Smaller, "shower" emboli tend to lodge in the peripheral subsegmental arteries, while larger masses get stuck at the bifurcation of the main pulmonary artery. This distribution pattern is the reason why ventilation-perfusion scans are so effective at identifying the mismatch in flow compared to air intake.
An engaged synthesis on vascular vigilance
We must stop treating the lungs and the legs as separate clinical entities. The reality is that the pulmonary vasculature is merely the final destination for a disaster that was likely choreographed in the deep veins of the lower body. It is my firm conviction that our current diagnostic obsession with the chest often comes at the expense of ignoring the venous source, leading to a high rate of recurrence. A pulmonary embolism is not a lung disease; it is a vascular failure. If we do not aggressively hunt for the origin—whether it be in the iliacs, the axillary veins, or the classic femoral stretch—we are simply treating the smoke while the fire still rages. Let's be clear: the most common place for a PE to hide is in our own clinical blind spots and the refusal to scan beyond the obvious. Vigilance is the only tool that actually reduces mortality in this high-stakes game of hemostatic roulette.