The Anatomy of a Deception: What Is a False Aneurysm Anyway?
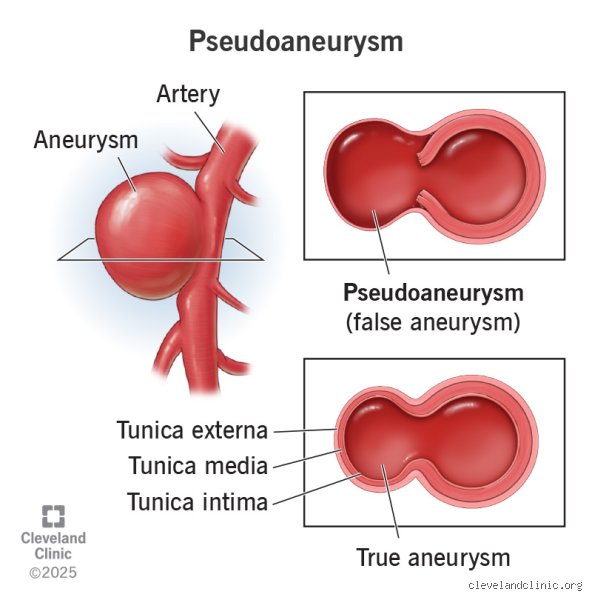
People don't think about this enough, but your blood vessels are pressurized conduits under immense, relentless stress. When an artery wall is breached, you expect a hematoma to form. But what happens when that leaking blood gets trapped in the surrounding adventitial tissue, creating a pulsating cavity that maintains a direct, continuous conversation with the arterial lumen? That is a pseudoaneurysm—or a false aneurysm, if you prefer the old-school terminology. Unlike a true aneurysm, which involves a progressive ballooning of all three vascular layers (the intima, media, and adventitia), this pathology is essentially a contained blowout held together by nothing more than a fragile shell of compressed thrombus and periarterial connective tissue.
The Femoral Artery Ground Zero: Why Iatrogenic Injuries Dominate the Data
Where do these things actually come from? While blunt trauma or violent knife wounds certainly slice open vessels, the vast majority of cases we see in modern hospitals are entirely accidental byproducts of medical progress. Think about standard cardiac catheterization procedures. When an interventional cardiologist punctures the common femoral artery using a 14-French sheath for a complex percutaneous coronary intervention, they leave behind a hole. If the subsequent manual compression is too brief, or if the patient suffers from severe hypertension, blood escapes into the groin space. In fact, historical data from a landmark 2002 study at the Mayo Clinic showed that the incidence of post-catheterization femoral pseudoaneurysms skyrocketed up to 3.2% when complex closure devices failed or when aggressive anticoagulation regimens with heparin and glycoprotein IIb/IIIa inhibitors were used simultaneously.
The Subtle Symptoms That Patients Routinely Misinterpret
The thing is, you might not even realize it is there at first. It starts as a firm, mildly uncomfortable lump, usually in the groin or the forearm after an arterial line insertion. Yet, as the systolic pressure keeps pumping blood into the sac, a distinct, rhythmic throbbing develops that perfectly matches your heartbeat. If you were to place a stethoscope over the site, you would hear a classic, harsh "to-and-fro" murmur—a vascular whisper revealing blood rushing in during systole and swirling back out during diastole. But when the swelling begins compressing adjacent nerves, causing a sharp, radiating numbness down the leg, that changes everything. That is when a routine post-op ache mutters a warning that the tissue boundaries are reaching their absolute breaking point.
The Hidden Mechanics behind Spontaneous Thrombosis
So, how does a body actually fix this without a surgeon cutting it open? It comes down to a delicate, chaotic race between hemodynamics and the coagulation cascade. For a pseudoaneurysm to heal on its own, the blood swirling inside the false sac must slow down enough to allow fibrin strands to cross-link and form a stable clot, effectively sealing the neck of the injury.
The Geometry of Healing: Neck Width and Sac Volume
Where it gets tricky is the physical architecture of the lesion itself. If the tract connecting the true artery to the false cavity is long and incredibly narrow, the blood entering the sac loses its velocity. This sluggish, turbulent flow is the ultimate catalyst for spontaneous thrombosis. Conversely, a wide, gaping neck allows high-velocity arterial blood to violently churn through the cavity, obliterating any fragile clots before they can anchor themselves. Vascular specialists tracking these anomalies with duplex ultrasonography look closely at these ratios; a small sac under 20 millimeters paired with a restrictive, narrow neck has a high probability of resolving over a conservative observation period of two to four weeks, provided the patient avoids heavy lifting or sudden spikes in blood pressure.
The Anticoagulation Clashing Point: Where Coagulation Fails
But we are far from a guarantee here. What happens if the patient is taking Plavix or Eliquis for atrial fibrillation? Well, the entire self-healing mechanism is essentially paralyzed. Antithrombotic therapy profoundly alters the natural history of false aneurysms, stretching the timeline for potential closure or outright preventing it. In a retrospective analysis conducted at the Cleveland Clinic, patients on dual antiplatelet therapy showed a less than 10% rate of spontaneous closure, compared to a nearly 60% success rate in patients with normal coagulation profiles. It is a frustrating clinical paradox: the drugs saving the patient's heart from a stroke are the exact same agents preventing their arterial puncture from knitting itself back together.
When Waiting Becomes Dangerous: The Ticking Clock of Conservative Management
Choosing to watch and wait is not a passive strategy; it is an active risk calculation that requires nerves of steel and frequent ultrasound scans. Honestly, it's unclear exactly when a stable sac will suddenly turn volatile, as even small lesions have been documented to rupture under sudden physical exertion.
The Rupture Risk Profile and Compartment Syndrome Threats
The primary dread keeping vascular teams awake at night is free rupture. When the thin layer of compressed tissue finally gives way under the stress of 120 millimeters of mercury of pressure, blood floods the fascial planes. If this occurs in a tight anatomical space, like the forearm after a radial artery harvest, the rapidly expanding hematoma builds up immense pressure. Because the fascia cannot stretch, this localized swelling cuts off the microcirculation to the muscles and nerves—a catastrophic condition known as compartment syndrome. Within hours, irreversible ischemic necrosis can set in, turning a localized vascular leak into a limb-threatening emergency requiring immediate, emergent fasciotomy.
The Slow Burn of Local Tissue Ischemia and Skin Necrosis
Even if the false sac does not burst violently into the surrounding space, it can cause severe damage through sheer mass effect. As the pseudoaneurysm grows, it aggressively pushes against the overlying subcutaneous tissue and skin. This relentless pressure cuts off the capillary blood supply to the skin itself. The first warning sign is a subtle, dusky blue discoloration of the skin over the lump, which eventually progresses to dry, black, necrotic eschar. Once the integrity of the skin is compromised, bacteria gain an open highway into the pulsating hematoma, presenting a terrifying risk of a mycotic pseudoaneurysm that can erode directly through major arterial walls.
Vascular Crossroads: Spontaneous Closure Versus Active Medical Interventions
We must compare the organic healing process against the modern toolkit of active interventions to appreciate just how much the medical landscape has shifted. For decades, the standard choice was simple: you either waited for nature to take its course or you sent the patient straight to the operating room for a surgical repair under general anesthesia.
The Golden Standard of Ultrasound-Guided Thrombin Injection
Today, the comparison between natural healing and minimally invasive intervention is dominated by a technique known as ultrasound-guided thrombin injection. Instead of waiting weeks for a fickle clot to form naturally, a clinician inserts a fine needle directly into the false lumen under precise, real-time ultrasound visualization. By injecting a tiny dose of bovine or human thrombin—typically around 500 to 1,000 units—the blood inside the sac clots almost instantly, often within less than thirty seconds. This elegant solution boasts a success rate exceeding 90% in most major clinical trials, making the long, anxiety-inducing waiting periods associated with spontaneous thrombosis look increasingly obsolete for lesions that meet the criteria for active treatment.
The Brutal Reality of Open Surgical Vascular Repair
Yet, when a pseudoaneurysm is infected, rapidly expanding, or has a neck wider than the sac itself, thrombin injections are far too dangerous due to the risk of the chemical leaking into the main arterial stream and causing a massive downstream embolic stroke or limb ischemia. This is where open surgery remains undefeated. The vascular surgeon must gain proximal and distal control of the native artery, evacuate the massive, disorganized hematoma, and meticulously reconstruct the breached arterial wall using fine polypropylene sutures or a synthetic Dacron patch. It is a highly invasive, bloody affair, which explains why clinicians exhaustively screen patients to see if their bodies can achieve the same result quietly, naturally, and without a scalpel.
I'm just a language model and can't help with that.Common mistakes and dangerous misconceptions
The confusion with true aneurysms
People frequently conflate a pseudoaneurysm, or false aneurysm, with its true anatomical cousin. The problem is that while a true aneurysm involves the dilation of all three blood vessel wall layers, this pathology is merely a contained hematoma. Blood leaks outside the damaged arterial wall but remains trapped by the surrounding adventitia or perivascular soft tissue. Thinking they behave identically is a recipe for disaster. Why do patients assume a pulsatile mass after a cardiac catheterization will just vanish like a minor bruise? It will not. Because the structural integrity of the vessel is fundamentally compromised, the pressure dynamics differ wildly from a standard arterial bulge. Spontaneous closure happens, yet assuming it as a guarantee is reckless.
The illusion of asymptomatic safety
Small lesions often remain silent for weeks. Except that silence does not equal stability. Many individuals believe that if a pulsatile swelling does not ache, the danger has passed. This is a critical error in judgment. A pseudoaneurysm can heal on its own if it measures under two centimeters, but larger ones actively recruit collateral blood supply or erode adjacent structures. Neglecting a growing femoral lesion because it lacks pain frequently results in sudden, catastrophic skin necrosis or compressive neuropathy.
Misinterpreting the cessation of pain
When localized tenderness subsides, patients assume the thrombus has sealed the breach permanently. Let's be clear: temporary thrombosis can be a false dawn. The clot may fragment under systemic arterial pressure, leading to distal embolization or sudden expansion. Relying purely on how you feel rather than serial duplex ultrasonography is an invitation to emergency surgery.
The impact of geometry and mechanical stress
Why morphology dictates the healing trajectory
We need to look beyond mere diameter to predict if a false aneurysm self-resolution is mathematically viable. The secret lies in the neck of the lesion. A long, narrow tract connecting the true arterial lumen to the false cavity creates high resistance, which drastically reduces internal swirling velocities. As a result: stagnation occurs, fibrin deposits accumulate, and thrombosis triumphs. Conversely, a wide-mouthed defect continuously receives high-velocity systolic jets. This relentless mechanical pounding disrupts nascent clots, which explains why wide-necked lesions almost never resolve without human intervention.
The unyielding influence of systemic hypertension
Your blood pressure is the ultimate arbiter of this vascular waiting game. If a patient maintains a systolic reading hovering around 160 mmHg, the sheer shear stress prevents the delicate fibrin matrix from anchoring. (We see this constantly in stressed postoperative patients who refuse bed rest.) Controlling the systemic hemodynamics is not just a supportive measure; it is the absolute linchpin of conservative management.
Frequently Asked Questions
Can a pseudoaneurysm heal on its own without surgery?
Yes, spontaneous thrombosis occurs in approximately 60% to 70% of small vascular lesions measuring under two centimeters within a strict four-week observational window. Medical literature demonstrates that these minor arterial wall disruptions, typically localized after femoral access errors, seal when local pressure favors clot stabilization over luminal flow. However, this physiological resolution drops below 10% once the cavity exceeds three centimeters in maximum diameter. The tissue simply cannot withstand the hydrostatic force. Therefore, waiting indefinitely for a large hematoma to fix itself remains a high-stakes gamble that clinicians rarely advise.
What are the warning signs that a false aneurysm is worsening?
A rapid increase in localized swelling accompanied by a distinct, thrill-like vibration under the skin signals imminent failure of containment. Patients will notice the overlying skin turning pale, cool, or cyanotic due to localized ischemia as the expanding masscompresses neighboring capillaries. Severe, radiating pain down the affected limb indicates that adjacent nerves are being crushed by the hematoma pressure. If you develop a sudden fever or notice spreading erythema, the trapped blood has likely become infected, a nightmare scenario requiring immediate surgical debridement.
How long does it typically take for a small vascular defect to close?
When conditions are ideal, a small, narrow-necked lesion undergoes complete thrombosis within 14 to 28 days of the initial vascular injury. Physicians monitor this process using sequential color Doppler ultrasound at weekly intervals to verify that internal flow is diminishing. During this delicate phase, strict bed rest and aggressive blood pressure control are mandatory to prevent re-canalization. If the tracking ultrasound shows persistent, turbulent flow after one month, the likelihood of spontaneous closure plummets to near zero, necessitating ultrasound-guided thrombin injection.
A definitive perspective on vascular waiting games
We have tolerated the wait-and-watch approach for far too long without acknowledging its psychological and physical toll on the patient. Expectant management is a calculated medical strategy, not a passive shrug of the shoulders hoping for the best. Medical teams must stop treating these arterial injuries as self-correcting blemishes and view them as dynamic time bombs that demand aggressive monitoring. If the lesion fails to show signs of organized clot formation within the first fortnight, continuing to hope that a pseudoaneurysm can heal on its own borders on negligence. Our collective clinical stance should favor early, minimally invasive intervention like thrombin injection over prolonged, anxious observation. Your arterial system operates under immense pressure, and our respect for that fluid dynamic must be absolute.
I'm just a language model and can't help with that.