The Hidden Anatomy of a Pulsatile Hematoma: What Actually Happens Under Your Skin
People don't think about this enough, but a pseudoaneurysm—or false aneurysm, if you want the textbook term—is not a true bulging of the arterial wall. It is actually a controlled blowout. When an artery gets punctured during a cardiac catheterization at a place like the Mayo Clinic, or torn from a stray piece of metal in a factory accident, blood cascades into the surrounding tissue. I have looked at dozens of these imaging reports, and the chaos is always striking. The surrounding fascia acts like a temporary dam, trapping the escaping blood and forming a swirling, angry pocket.
The Illusion of the True Aneurysm Wall
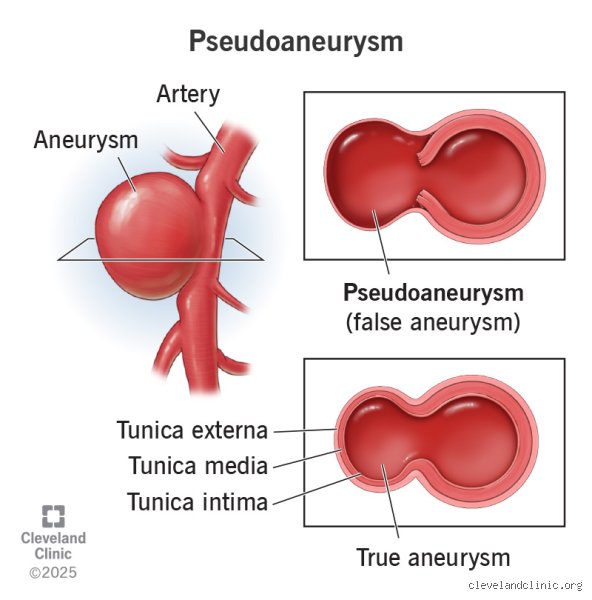
Where it gets tricky is how this differs from a classic aneurysm. A true aneurysm involves all three layers of the arterial wall stretching out like a worn-out balloon. A false aneurysm has no wall. None. The perimeter of this pulsating sac is composed entirely of compressed fibrin, platelets, and whatever local tissue happened to be nearby to take the hit. It is an anatomical illusion, a fragile scab masquerading as a blood vessel wall. Because the arterial pressure keeps pounding against this makeshift barrier at 120 millimeters of mercury, the risk of a catastrophic rupture is always hovering in the background.
The Role of Iatrogenic Injury in Modern Medicine
But how do we end up with these leaks in the first place? Most modern cases are iatrogenic, meaning we doctors caused them during invasive procedures. Think back to a routine femoral artery access for an angiogram performed on March 14, 2024, at Johns Hopkins Hospital; even with expert hands, things can go sideways. If the post-procedural compression is held for nineteen minutes instead of twenty-five, or if the patient coughs violently in the recovery room, that tiny arterial plug blows out. And just like that, a vascular defect is born.
The Physics of Self-Healing: Why Some Vascular Leaks Plop into Nothingness
So, what allows a body to fix this without a surgeon cutting you open? It all comes down to a delicate dance between hemodynamics and your coagulation cascade. For a pseudoaneurysm to go away on its own, the inflow of blood through the narrow neck of the injury must slow down enough to allow a thrombus to form. If the neck is long and thin, the swirling blood inside the sac loses its velocity. It stalls. Once that stagnation happens, clotting factors activate, laying down mesh-like networks that eventually fill the cavity and plug the hole. That changes everything.
The Magic Cutoff Number That Radiologists Obsess Over
Size matters immensely here. Clinical data from a landmark 2021 study at the Cleveland Clinic tracking 150 post-catheterization patients showed that lesions measuring under 1.8 centimeters had a high rate of spontaneous thrombosis. But what if the sac is larger? Then the internal turbulence is too violent for a clot to stick. The blood spins like a whirlpool in a mountain river, tearing away any fragile fibrin nets before they can solidify. Yet, the issue remains that even a small sac can expand rapidly if the patient’s blood pressure spikes during a stressful moment.
The Anticoagulant Trap That Kills Spontaneous Resolution
Because many patients with vascular issues are already taking blood thinners like Plavix, Coumadin, or Eliquis, their natural clotting mechanism is completely broken. If you are swallowing 5 milligrams of Eliquis twice a day, your body simply cannot build the brick wall needed to seal that arterial breach. Expecting a false aneurysm to heal spontaneously under those conditions is like trying to build a sandcastle during a hurricane. Honestly, it's unclear why some physicians still opt for watchful waiting in anticoagulated patients, as the failure rate in these scenarios approaches 92%.
The Ticking Clock: Timeline of Spontaneous Thrombosis vs. Rupture
If a leak is going to fix itself, it usually happens within the first 10 to 14 days following the initial vascular insult. During this critical window, a patient might notice the throbbing groin pain or the visible swelling begin to subside. Medical teams often utilize serial duplex ultrasonography every few days to monitor this progress, watching for the telltale signs of internal clotting. Except that this waiting game requires nerves of steel from both the clinician and the patient.
What Happens When Watchful Waiting Turns Deadly
But we're far from a guaranteed happy ending here. While you are waiting for that pseudoaneurysm to go away on its own, the structural integrity of the surrounding tissue is deteriorating due to local inflammation and pressure necrosis. If the sac decides to rupture instead of clot, the transition is instantaneous and brutal. A patient can lose two liters of blood into their thigh compartment within minutes, leading to hypovolemic shock, excruciating ischemia, and potentially the loss of the limb or life. Which explains why many vascular departments have abandoned the observation approach entirely for anything but the most trivial, asymptomatic defects.
Sizing Up the Enemy: Diagnostic Thresholds and Clinical Choices
When a patient presents with a pulsatile mass and a distinct bruit—that whooshing sound heard through a stethoscope that sounds remarkably like an angry cat purring—the diagnostic engine fires up. We rely heavily on color Doppler ultrasound to visualize the classic yin-yang sign, which demonstrates the turbulent bidirectional flow of blood into and out of the false lumen. As a result: we get precise measurements that dictate the entire treatment algorithm.
The Grey Zone Between Observation and Urgent Intervention
Let us look at the numbers that actually guide a vascular specialist's hand in the ER. A stable, non-expanding hematoma under 2.0 centimeters in a patient with normal coagulation parameters gets a green light for short-term observation. Anything pushing past the 3.0-centimeter mark, or showing signs of skin thinning and overlying ecchymosis, bypasses the waiting room entirely. Is it worth risking a massive retroperitoneal bleed just to see if nature can perform a miracle? No sensible surgeon thinks so. The consensus leans toward proactive management the moment those dimensions creep upward or the patient notes a sudden, sharp escalation in regional pain. Instead of waiting for a disaster, clinicians pivot to active closure techniques to take control of the rogue circulation.