The Great Realignment of Oral Healthcare Infrastructure
We often talk about healthcare as a unified front, yet dentistry routinely gets shoved into a separate, oddly capitalistic bucket. The thing is, oral care is treated as a luxury luxury until an infection hits your bloodstream. Across the globe, the World Health Organization recommends a baseline ratio of one practitioner per 2,000 people, but this metric is deeply flawed. Why? Because it completely ignores geography.
The Statistical Illusion of the Dentist-to-Patient Ratio
Take France or Australia, for instance. On paper, their national aggregates look perfectly healthy, even comfortable. Yet, when you zoom into the regional realities of places like the rural Occitanie region or the Australian Outback, the numbers plummet into terrifying territory. A country can possess a glowing national average while its rural citizens are pulling their own teeth out with pliers in desperation. People don't think about this enough: a high concentration of cosmetic specialists in a wealthy metropolis like Paris or New York does absolutely nothing for a toddler with rampant caries three hundred miles away.
Defining the Modern Shortage Matrix
A true systemic deficit occurs when the state-subsidized system fails to retain professionals, driving them into exclusively private, out-of-pocket cosmetic work. When analyzing global dental provider deficits, we must differentiate between an absolute lack of trained professionals—which defines much of the developing world—and an economic migration away from public health contracts. This latter phenomenon is exactly what is currently paralyzing the British Isles, turning routine check-ups into a privilege reserved for the affluent.
The British Collapse: A Deep Dive into the NHS Crisis
Let us look closely at the United Kingdom, because that changes everything we thought we knew about Western medical supremacy. The British situation is not just bad; it is arguably the most dramatic breakdown of public oral healthcare in a G7 nation since the inception of the welfare state. By the start of 2026, data revealed that over 80% of dental practices across England were no longer accepting new adult NHS patients. Think about that for a second.
The Ghost of the 2006 Contract and the Great Exodus
The root of this catastrophe lies in a piece of bureaucratic legislation passed two decades ago—the infamous 2006 NHS dental contract. This system rewards dentists using Units of Dental Activity (UDAs), a bizarre metric where a practitioner receives the same financial reimbursement whether they perform a single, simple filling or a complex, three-hour root canal reconstruction on a patient who has not seen a doctor in ten years. The math simply stopped working. As a result: clinic owners started losing money on every public patient they treated. I spoke with a clinic director in Norfolk recently who admitted that transitioning to a 100% private model was the only way to avoid bankruptcy, even though it meant abandoning thousands of vulnerable local pensioners.
The Rise of Do-It-Yourself Dentistry in Regional England
What happens when a town loses its last public clinic? The situation turns dystopian very quickly. In places like West Cumbria or Devon, charities like Dentaid—which traditionally operated in refugee camps and developing nations—now deploy mobile vans to the streets of British towns to treat citizens who cannot afford private fees. A 2025 British Dental Association poll shocked the public by revealing that one in ten respondents had attempted some form of DIY dentistry, using superglue to secure crowns or purchasing temporary filling kits online. It sounds like something out of a Dickens novel, yet it is happening in the world's sixth-largest economy. The issue remains that the government refuses to fundamentally restructure the UDA system, offering instead minor band-aids that fail to stem the bleeding.
The North American Divide: Geographic Deserts in the US and Canada
Across the Atlantic, the narrative shifts from broken state contracts to raw economic exclusion and vast geographic distances. Here, the phrase maldistribution of dental professionals takes on an entirely different meaning, dictated by corporate consolidation and massive student debt loads.
The Million-Dollar Debt Trap Driving American Specialization
The average American dental student graduates owing more than $300,000, a staggering financial burden that dictates their entire career trajectory. Where it gets tricky is the repayment strategy. Can you blame a twenty-six-year-old graduate for bypassing a low-income clinic in rural Mississippi or New Mexico when they can join a corporate dental conglomerate in a wealthy suburb of Dallas or Atlanta? Obviously not. This economic reality has created massive Dental Health Professional Shortage Areas (HPSAs) across the United States. According to the Health Resources and Services Administration, as of late last year, over 70 million Americans reside in areas without adequate access to oral care, requiring the addition of roughly 12,000 practitioners to eliminate the deficit.
Canada’s Rural North and the Failure of Universal Care Expansion
Canada presents its own unique paradox. While Ottawa launched the Canadian Dental Care Plan (CDCP) to expand coverage to millions of uninsured residents, the policy hit a massive snag: you cannot provide care if there are no clinics to accept the insurance. In the northern territories like Nunavut, the shortage is catastrophic, with some communities relying entirely on fly-in practitioners who visit once or twice a year. Except that flying a professional into an Arctic community for four days does not solve chronic, structural periodontal disease. The rollout of the CDCP has actually exacerbated the visible friction between urban abundance and rural neglect, proving that funding insurance without expanding the physical workforce is an exercise in futility.
Global Comparisons: Public vs. Private Shortage Dynamics
To truly understand which country has a shortage of dentists, we have to look at how different national models hold up under economic strain. Experts disagree on whether a highly regulated state model or a pure market system yields better access, and honestly, it’s unclear because both seem to fail specific demographics spectacularly.
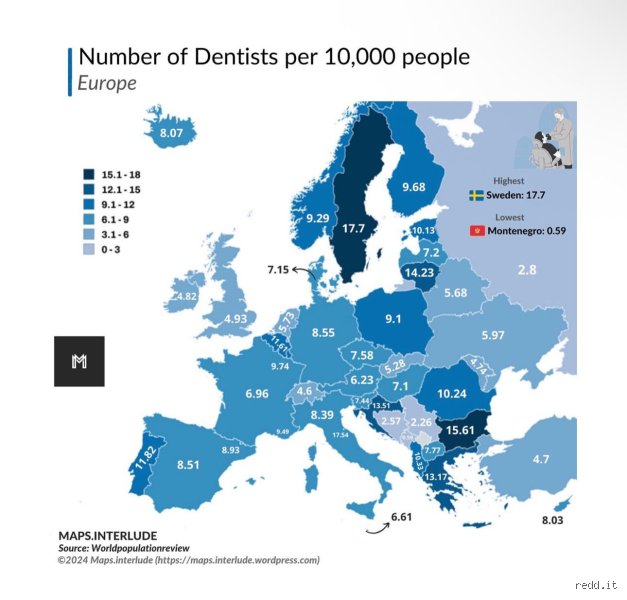
The Nordic Insulation vs. Southern European Surplus
Look at Scandinavia. Countries like Sweden and Denmark boast some of the highest provider densities globally, heavily subsidized by state funds and integrated into school systems from early childhood. But even there, the system is showing cracks as aging populations require more complex geriatric care. Meanwhile, Spain and Greece have an oversupply of graduates, which explains why many Iberian practitioners migrate north to the UK or Germany, chasing better wages and fleeing an oversaturated domestic market where young professionals end up working as underpaid assistants. It is a striking contrast: a continent where one corner is starving for extractions while the other has graduates driving Ubers.
The Critical Voids of the Global South
But let us maintain some perspective here, because the shortages in the West, as painful as they are, pale in comparison to the absolute vacuums of the Global South. In nations like Ethiopia, Malawi, or Niger, the ratio frequently exceeds one provider per 250,000 individuals. In these regions, a dental infection is not an expensive inconvenience or a long wait on a phone line; it is a life-threatening condition that can lead to severe systemic sepsis without any surgical intervention available. In short, while the UK suffers from an administrative and economic shortage, these nations face an existential absence of infrastructure, a reality that the international community routinely ignores.
Common mistakes and dangerous misconceptions
The "more graduates equals fewer cavities" fallacy
You probably think churning out a fresh battalion of dental school graduates solves the issue overnight. It does not. Look at France, where the state regulated student quotas tightly for decades. They recently loosened the valves, yet rural areas remain completely barren of practitioners. Why? Because newly minted professionals refuse to set up shop in isolated towns, preferring the comfortable oversaturated urban hubs instead. We are treating a structural distribution disease with a raw volume band-aid. The problem is that a diploma does not dictate geographical destiny.
Equating raw dentist-to-population ratios with actual access
Let's look at the numbers closely. A country might boast a seemingly healthy statistic of 70 practitioners per 100,000 citizens on paper, masking a horrific reality. In Canada, urban centers are swimming in clinics, but northern indigenous communities suffer from a severe lack of oral healthcare professionals. Except that people love averages because they hide uncomfortable truths. A national average is a statistical ghost that comforts politicians while citizens wait thirteen months for a basic root canal. Which country has a shortage of dentists? It is often the very one bragging about its aggregate medical registry data.
Assuming private insurance solves systemic scarcity
The United States serves as a brutal case study here. Having excellent corporate dental benefits means absolutely nothing if the nearest available provider is a three-hour drive across state lines. Medicaid reimbursement rates for pediatric oral procedures are so laughably low that private clinics simply lock their doors to low-income families. As a result: thousands of children rely on emergency rooms for preventable abscesses. Wealth cannot buy a service that physically does not exist in your zip code.
The hidden driver: Corporate dental monopolies and clinical burnout
The quiet death of the independent local practice
Have you noticed your local clinic suddenly changing its name to a generic corporate brand? Private equity firms are aggressively swallowing independent practices across the United Kingdom and Australia. They optimize for maximum profit margins, which explains why seasoned practitioners are fleeing the industry in droves. Young associates are saddled with astronomical student debts, often exceeding $300,000 in the American system, forcing them into these high-pressure corporate assembly lines. They are pushed to upsell cosmetic veneers rather than performing basic preventative care for the needy.
The licensing wall: Why foreign credentials gather dust
Here is a deeply frustrating paradox. Thousands of highly qualified immigrant practitioners are currently driving Uber in Toronto and London. Bureaucratic protectionism forces them to endure years of redundant, prohibitively expensive retraining programs before they can touch a mirror. The issue remains that we choose protection of professional guilds over public health necessity. But altering these deeply entrenched protectionist laws requires political courage that is currently nowhere to be found.
Frequently Asked Questions
Which country has a shortage of dentists that impacts rural populations most severely?
Australia faces a massive crisis where the geographic maldistribution of its 17,000 registered practitioners leaves outback territories in total neglect. While Sydney and Melbourne enjoy a surplus of one practitioner per 1,200 people, remote areas suffer through a ratio of one to 5,500 residents. The government attempted to fix this by offering regional practice subsidies, but the allure of metropolitan private cosmetic clinics consistently wins. Consequently, rural Australians experience tooth extraction rates that are double those of their urban counterparts. It proves that geographic isolation amplifies the deficit of dental practitioners far more than simple national averages suggest.
How does the crisis manifest within European healthcare models?
The United Kingdom serves as the most prominent European example where the National Health Service dental framework has effectively collapsed. Recent British Dental Association data revealed that 90% of NHS practices across the country were refusing to accept new adult patients for routine treatment. This massive institutional failure has birthed the horrific phenomenon of "DIY dentistry," where desperate citizens use superglue and hardware pliers to extract their own teeth. The state insurance system underpays clinics for complex operations, which induces practitioners to abandon public contracts entirely to pursue lucrative private cosmetic work. In short, a universal healthcare system on paper means nothing when the state budget refuses to fund real-world operating costs.
Can dental therapists and hygienists permanently solve this global bottleneck?
Expanding the scope of mid-level providers offers a temporary relief valve, but it cannot fully replace specialized surgical expertise. Countries like New Zealand have successfully utilized advanced dental therapists to manage pediatric fillings and preventative cleanings in schools since the last century. This frees up university-trained professionals to tackle complex maxillofacial pathologies and intricate reconstructive surgeries. However, powerful medical lobbies in various nations actively fight these scope-of-practice expansions to protect their financial monopolies. Ultimately, we must recognize that while a hygienist can clean a tooth, they cannot safely manage a deep jaw bone infection or reconstruct a shattered mandible.
A radical reappraisal of oral healthcare infrastructure
We must stop treating oral health as a luxury cosmetic add-on to human biology. The separation of dentistry from general medicine is a historical mistake that continues to kill people via systemic infections and preventable cardiovascular complications. (Let's be clear: your teeth are not independent of your bloodstream.) If we continue to allow private equity firms to dictate where clinics open and which procedures are prioritized, the global scarcity of dental specialists will transform from a chronic inconvenience into a public health catastrophe. Governments must aggressively conscript subsidized students into mandatory rural service, break the protectionist licensing monopolies that bar foreign experts, and tie public funding to geographical equity. Anything less than a total systemic overhaul is just performative political theater while a generation's teeth rot away.