The Neurological Illusion: Why Your Brain Misinterprets the Signal
Pain is not a direct phone line from your stubbed toe to your consciousness. The old Cartesian model of biology—the one stating that an injury equals an exact amount of suffering—is completely dead, yet people still cling to it. When an injury occurs, peripheral nerves send a cascade of electrochemical impulses up the spinothalamic tract toward the thalamus, which acts as a grand central sorting station. But here is where it gets tricky. The thalamus forwards this raw data to the primary somatosensory cortex for localization, but it also floods the anterior cingulate cortex and the amygdala, which handle emotion and fear. The brain actually constructs the sensation of pain based on memory, expectation, and current emotional threat levels rather than raw tissue damage.
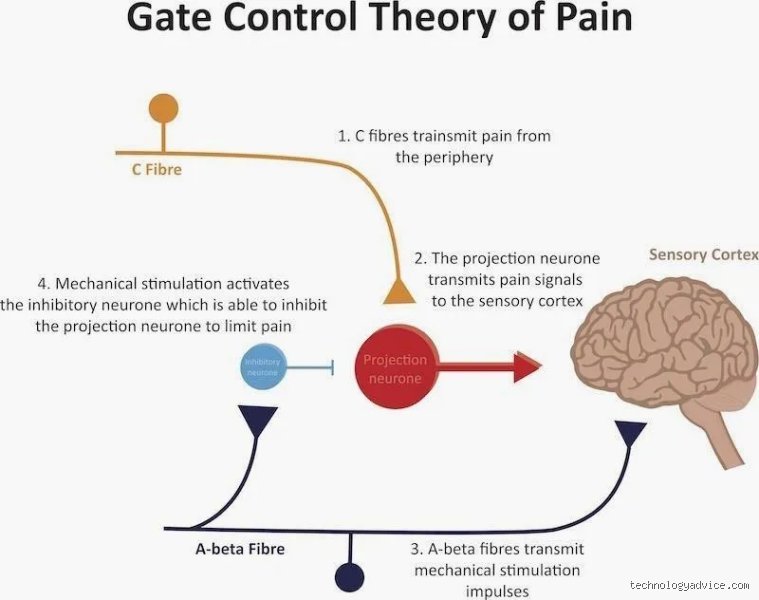
The Gate Control Theory of 1965 and Why It Still Matters
Ronald Melzack and Patrick Wall revolutionized medicine at MIT when they realized that psychological factors can physically close a neural "gate" in the dorsal horn of the spinal cord. If you are anxious, the gate swings wide open, amplifying the signal; conversely, if you can flood the nervous system with competing cognitive tasks or deep relaxation, you slam the gate shut. Think of it like a crowded highway where cognitive distractions act as a roadblock, preventing the distress signals from reaching awareness. It is an imperfect filter—experts disagree on the exact synaptic mechanics of chronic states—but the core premise remains undisputed. If you change the cognitive context, you change the physical sensation.
Deconstructing the Somatosensory Network Through Cognitive Decoupling
To pull off this mental magic trick, you have to master cognitive decoupling. This is the deliberate practice of separating the objective physical sensation (the raw data) from the emotional evaluation of that sensation (the suffering). When a migraine strikes, the natural human response is a cascade of panic—"How long will this last? I can't do my job today"—which triggers a massive release of cortisol and adrenaline. That changes everything, and not for the better, because those stress hormones explicitly lower your threshold for physical discomfort. By shifting into a radical state of objective observation, you strip the emotional power away from the neural pathway.
The Stanford Protocol and Somatosensory Focus
In a landmark 2005 study at Stanford University, researchers utilized real-time functional magnetic resonance imaging (rt-fMRI) to show that individuals could consciously control the activation of their rostral anterior cingulate cortex. Participants stared at a visual representation of their own brain activity—rendered on a screen as a flickering flame—and used cognitive reappraisal to shrink the fire. It worked remarkably well. But how do you do this without a multi-million-dollar scanner? You begin by analyzing the discomfort as if you were a detached scientist observing a specimen under a microscope. Is it hot or cold? Does it vibrate, or is it a steady throb? Is the perimeter sharp, or does it bleed into the surrounding muscle? By translating the experience into neutral, descriptive data points, the amygdala stops treating the sensation as an existential threat, and the perceived intensity drops precipitously.
The Power of Radical Sensory Substitution
Another weapon in the cognitive arsenal is sensory substitution, a technique frequently used by elite athletes to endure extreme physical exertion. Instead of trying to ignore a burning sensation in a muscle, a marathoner might consciously reframe that exact neurological signal as a sensation of intense, cool pressure or even a benign electrical current. Honestly, it is unclear why the brain accepts these arbitrary reassignments so readily, but the clinical efficacy is undeniable. The nervous system struggles to process two conflicting interpretations of the same sensory input simultaneously, forcing it to default to the framework you consciously reinforce.
The Autonomic Reset: Hijacking the Vagus Nerve to Mute the Alarm
You cannot think your way out of a physical crisis if your sympathetic nervous system is screaming at maximum volume. This is where the vagus nerve becomes your best friend. As the main superhighway of the parasympathetic nervous system, the vagus nerve regulates your heart rate, digestion, and immune responses. When you are in agony, your breathing becomes shallow, your heart rate variability plummets, and your body enters a hyper-vigilant state that actually primes your brain to feel more discomfort. Breaking this feedback loop requires a deliberate, mechanical intervention to trick your physiology into a state of deep safety.
Resonant Frequency Breathing and the 5.5-Second Rule
The fastest way to trigger a vagal reset is through resonant frequency breathing, which involves inhaling for exactly 5.5 seconds and exhaling for 5.5 seconds, totaling roughly six breaths per minute. This specific cadence maximizes heart rate variability and stimulates the baroreceptors in your carotid sinuses. As a result: the brain receives an immediate signal that the physical body is completely safe, causing the hypothalamus to halt the production of pro-inflammatory cytokines. And because those cytokines are responsible for sensitizing peripheral nociceptors, reducing their presence directly blunts the physical sharpness of the distress signal. People don't think about this enough, but a calm body is biologically incapable of sustaining a high-intensity pain panic response.
Comparing Mental Deception to Pharmacological Alternatives
It is worth comparing these self-directed cognitive interventions against traditional pharmacological approaches like acetaminophen, NSAIDs, or synthetic opioids. While a pill can block cyclooxygenase enzymes or bind to mu-opioid receptors in the brain, it represents a passive, blunt-force trauma approach to a highly nuanced neurological problem. Medications come with a hefty tax—gastrointestinal erosion, liver toxicity, cognitive clouding, and the terrifying specter of chemical dependency. Cognitive modulation, yet, relies on endogenous opioid production and descending inhibitory pathways without any metabolic hangover.
The Placebo Effect as a Legitimate Neurochemical Tool
We often dismiss the placebo effect as a trick, a psychological illusion that doesn't count as real medicine. We're far from it, though. When a patient takes a sugar pill believing it is a potent analgesic, their brain releases a massive wave of endogenous endorphins and enkephalins that physically block pain signals in the spinal cord. This is not imaginary; it is a demonstrable, chemical reality that can be blocked by administering naloxone, an opioid antagonist. This proves that the human mind possesses a built-in pharmacy capable of synthesis on demand. The issue remains that most people have never been taught how to open the cabinet door without a dummy pill to trigger the lock, a failure of modern medical education that leaves millions unnecessarily dependent on external substances.
Common Mistakes and Misconceptions When You Try to Mute Nociception
The Illusion of Total Eradication
Most novices attempt to construct a monolithic mental wall against their discomfort. They expect a total blackout. Except that the human nervous system does not possess a binary toggle switch. When you try to mentally turn off pain by sheer force of will, you inadvertently sharpen your focus on the very sensation you despise. It backfires. The brain interprets this aggressive resistance as a threat signal, which actually amplifies the dorsal horn signaling. Stop fighting the wave. Yielding to the sensation sounds counterintuitive, yet it diminishes the secondary emotional suffering that amplifies physical agony.
The Trap of Toxic Positivity and Forced Distraction
Plastering a superficial smile over a agonizing migraine is a recipe for neurological exhaustion. Distraction works, but only up to a threshold of approximately 4 out of 10 on the visual analog scale. Beyond that? Your amygdala sees right through the charade. Why do we keep trying to trick a survival mechanism that has evolved over millions of years? The problem is that suppression breeds obsession. If you tell your subconscious to ignore a throbbing toothache, it monitors that toothache with increased vigilance to ensure your survival. Instead of pretending the discomfort is absent, acknowledge its presence without assigning a catastrophic narrative to it.
Misunderstanding the Timeline of Neuroplasticity
Expectations ruin progress. Changing how your cortex processes nociceptive input requires physical remodeling of synaptic pathways. It takes time. Because a single meditation session failed to blunt your chronic lower back discomfort, you assume the methodology is faulty. That is like lifting weights for twenty minutes and expecting Olympic musculature. Cortical reorganization demands relentless, daily repetition before the grey matter changes density in the anterior cingulate cortex.
The Somatosensory Shift: An Expert Strategy for Deep Neuromodulation
Somatic Tracking and the Art of Objective Deconstruction
Let us be clear: you cannot think your way out of a broken femur, but you can radically alter how your brain decodes chronic, non-structural signals. The most potent tool in clinical psychology is somatic tracking. This involves objective, analytical observation. Instead of perceiving a massive, terrifying blob of suffering, map its precise borders. Is it hot or cold? Does it vibrate, or is it a steady pressure? By translating an emotional threat into cold, neutral sensory data, you strip the signal of its panic-inducing power. As a result: the prefrontal cortex dampens the alarm bells of the limbic system, shifting you from fight-or-flight into a state of physiological safety.
Consider a patient suffering from phantom limb sensations. By using a mirror box to visually trick the brain, we alter the somatosensory map. You can replicate this mentally. Imagine the boundaries of the discomfort shrinking by a mere two percent every ten minutes. It is a slow, meticulous dissolution. (Your internal monologue must remain as detached as a scientist monitoring a laboratory experiment). You are no longer the victim of the sensation; you are its observer. This subtle shift in identity alters the chemical cocktail bathed around your synapses, reducing substance P and increasing the flow of endogenous opioids.
Frequently Asked Questions Regarding Neural Pain Modulation
Can anyone truly learn how to mentally turn off pain completely?
Total elimination remains an elusive myth for the vast majority of the population, though significant mitigation is universally achievable. Clinical data from neuroimaging studies indicates that elite practitioners of Tibetan Tummo meditation can reduce their subjective distress ratings by up to 64 percent. This occurs through the conscious down-regulation of the primary somatosensory cortex during noxious thermal stimulation. For the average individual, achieving a 30 to 40 percent reduction in intensity is a highly realistic therapeutic goal. The issue remains that genetic variances in COMT and OPRM1 receptor expressions dictate your baseline capacity for endogenous opioid production, meaning results will always vary. In short, absolute mastery is rare, but substantial relief is accessible to any brain capable of focused neuroplastic training.
How does stress impact our ability to alter sensory perception?
Stress acts as a massive amplifier that sabotages your attempts to mentally turn off pain at the cortical level. When cortisol and adrenaline spike, the thalamus lowers its gating threshold, allowing a flood of sensory inputs to reach your conscious awareness. A study published in the journal Neurobiology of Disease demonstrated that high-stress cohorts exhibit a 45 percent reduction in their natural pain thresholds compared to relaxed control groups. This happens because chronic anxiety depletes the brain of serotonin and norepinephrine, two neurotransmitters necessary for the descending inhibitory pathway to function. You cannot expect to master your physical sensations while your mind is trapped in a chaotic loop of psychological panic.
Is it dangerous to suppress physical warning signals using the mind?
Silencing an acute warning signal without diagnosing its underlying cause is an incredibly perilous gamble. Acute discomfort is a protective biological imperative that prevents you from walking on a fractured ankle or ignoring an inflamed appendix. Medical literature documents cases of congenital insensitivity where individuals suffer severe tissue damage and shortened lifespans precisely because they lack these vital alarms. But chronic discomfort is an entirely different beast; it is a glitching software program rather than a helpful warning of structural damage. Once a physician has ruled out active tissue destruction or malignancy, actively working to dull that persistent feedback loop is not only safe but highly recommended for preserving cognitive function.
A Paradigm Shift in Conscious Suffering Management
We must stop treating discomfort as an invincible tyrant and start treating it as a flawed, malleable piece of neurological data. The western medical model has conditioned us to run to the pharmacy at the first hint of physical distress, which explains why we have forgotten the immense, latent power of our own endogenous descending inhibitory pathways. It is time to reclaim that autonomy. Do not expect an effortless victory or a magical mental eraser that cures all ailments instantly. Realism dictates that we acknowledge the biological limits of our meat suits. Yet, by methodically deconstructing our sensations and stripping them of emotional terror, we can comfortably coexist with conditions that previously broke our spirits. Take charge of your neural gating mechanisms because a life dictated by an overactive nervous system is no way to live.