Beyond the Prescription Pad: Why Single-Target Solutions Fail Miserably
For decades, the medical establishment chased a phantom.
Doctors behaved as if human suffering could be turned off like a kitchen faucet, provided you found the right chemical wrench. Except that it does not work that way, does it? The 3 P's of pain relief emerged precisely because the monotherapy model—relying solely on one treatment—collapsed under the weight of the late 1990s opioid epidemic, a disaster triggered by the over-prescription of heavy analgesics at clinics like the infamous structures in Broward County, Florida. We learned the hard way that masking a signal is not the same as curing the tissue.
The Biopsychosocial Shift in Modern Neurology
Pain is not just a localized fire burning in your lower back or your knee. In 1977, psychiatrist George Engel introduced the biopsychosocial model, which explains why two people with the exact same spinal disc herniation can experience entirely different levels of agony. One person might run a marathon; the other might be bedridden. Neurons do not fire in a vacuum, meaning that your emotional state, your sleep quality, and even your financial stress dictate how loudly your brain screams in response to a nerve signal.
Where the Mechanical View of Human Suffering Crumbles
The thing is, your nervous system possesses an annoying trait called neuroplasticity. When a nociceptive pathway is stimulated repeatedly over months, the brain actually gets better at processing that distress, lowering your tolerance threshold. Because of this rewiring, treating a chronic condition like fibromyalgia with nothing but a heating pad or a standard anti-inflammatory drug is like trying to put out a house fire with a squirt gun.
Pillar One: The Complex Reality of Pharmacology in Distressed Systems
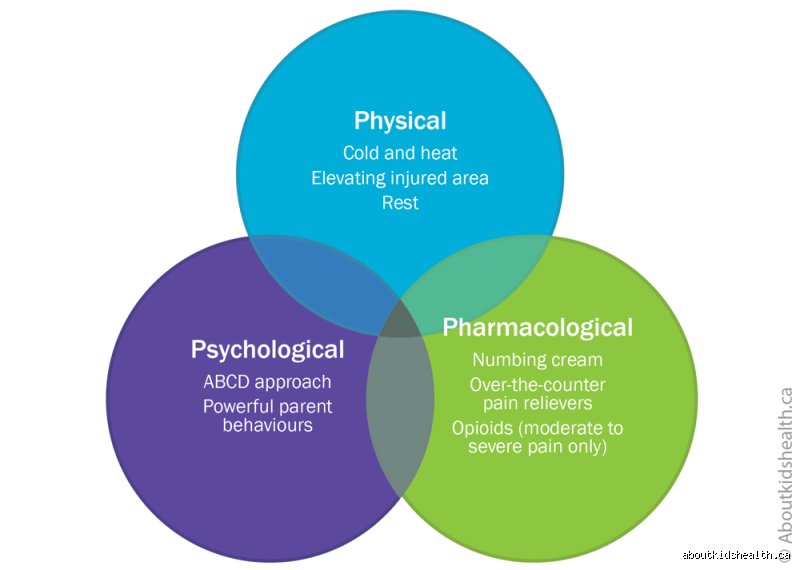
Let us look at the first component of the 3 P's of pain relief, which happens to be the most misused tool in the entire medical shed: pharmacology. It is the immediate fallback option for a reason. Medications offer rapid, measurable alterations in blood chemistry, yet the issue remains that their efficacy drops sharply over time while the side-effect profile climbs. I firmly believe that we cannot talk about chemical intervention without acknowledging that pills are often just a bridge, not the destination.
From Over-the-Counter Non-Steroidal Drugs to Neurological Modulators
Your local pharmacy shelves are packed with options, but people don't think about this enough: even basic over-the-counter drugs carry steep costs if abused. Acetaminophen remains the leading cause of acute liver failure in the United States, accounting for roughly 56,000 emergency room visits annually. When standard anti-inflammatories fail, clinicians often step up to gabapentinoids—like pregabalin—which do not target inflammation at all but instead quiet down overactive, misfiring voltage-gated calcium channels in the central nervous system. It is a highly sophisticated approach, though honestly, it's unclear why certain patients experience massive cognitive fog on these drugs while others feel completely normal.
The Delicate Balancing Act of Managing Receptor Tolerance
Mu-opioid receptor agonists represent the heavy artillery of the pharmacological world. They are unmatched for acute post-surgical trauma, but when used for chronic, non-cancer ailments, the cellular machinery rebels. Cells rapidly internalize these receptors, meaning you need higher doses to achieve the same baseline comfort, a trajectory that frequently leads to opioid-induced hyperalgesia—a paradoxical state where the medication actually makes you more sensitive to physical distress. Experts disagree on the exact timeline of this shift, but some clinical data suggests changes begin in as little as 14 days of continuous exposure.
Pillar Two: Physical Therapy and the Mechanics of Restorative Motion
Movement is medicine, but only if the dosage is correct. The second element of the 3 P's of pain relief shifts the focus from chemical manipulation to mechanical adaptation. Physical therapy is not about doing a few lazy leg lifts on a mat; it is a systematic restructuring of how your musculoskeletal system distributes load. If a joint is unstable, the surrounding muscles will spasm to create a artificial splint, causing a secondary wave of agony that people often mistake for the primary injury.
Targeted Kinesiotherapy Versus General Exercise Guidelines
There is a massive gulf between going for a walk and engaging in targeted kinesiotherapy designed by a specialist. Take chronic lower back issues, which affect an estimated 619 million people worldwide as of recent global health audits. A structured physical therapy regimen focuses heavily on eccentric strengthening of the multifidus muscle and stabilizing the transverse abdominis. This specific muscular armor decompresses the lumbar spine, which explains why passive modalities like ultrasound or passive stretching rarely provide lasting structural changes on their own.
Overcoming the Cycle of Fear-Avoidance and Muscle Atrophy
Here is where it gets tricky for the average patient. When movement hurts, your natural instinct is to stop moving entirely, a psychological trap known as the fear-avoidance belief model. This immobility causes rapid muscle atrophy and joint stiffness, which makes the next attempt at movement hurt even more. To break this loop, physical therapists utilize graded activity protocols, slowly introducing movement under the neurological radar so the brain realizes it can move without triggering a catastrophe.
Comparing Chemical Blockades with Active Physical Re-education
We need to compare these first two pillars directly because they operate on completely opposing philosophies. Pharmacology acts as a top-down chemical blockade, stopping signals from reaching awareness. Physical therapy, conversely, is a bottom-up mechanical re-education, altering the physical structures that generate those signals in the first place.
Immediate Chemical Relief Versus Sustained Functional Gains
If you take a 400-milligram tablet of ibuprofen, it begins inhibiting cyclooxygenase enzymes within roughly 30 minutes, lowering prostaglandin synthesis and giving you a window of comfort. That is a quick win. Sustained physical therapy, however, takes between 6 to 8 weeks of consistent compliance before visible myofibrillar hypertrophy and neural adaptations manifest. It demands patience that a hurting patient rarely possesses, as a result: many abandon the physical track far too early, retreating to the ease of the prescription bottle.
The Economic and Systemic Costs of Long-Term Strategies
Let us look at the raw financial metrics. A year of continuous advanced pharmacological management, especially involving branded neuropathic drugs or regular corticosteroid injections under fluoroscopic guidance, can easily top 5,000 dollars in out-of-pocket expenses. A structured, 12-week course of physical therapy might cost a fraction of that amount while simultaneously reducing the likelihood of future spinal surgeries by up to 50 percent, according to long-term orthopedic tracking studies. In short, one approach charges you indefinitely to manage the symptoms, while the other builds a physical shield against the return of the injury.
Common mistakes and misconceptions surrounding chronic management
The trap of passive reliance
You swallow a pill and wait for the magic to happen. The problem is, modern medicine has conditioned us to expect instant, effortless extinction of discomfort. Relying solely on pharmaceutical intervention ignores the structural reality of how human neurology processes suffering. When people treat the 3 P's of pain relief as a buffet where they can choose only the physical option, long-term rehabilitation fails. Passive modalities like heating pads or massage feel spectacular in the moment, except that they rarely reprogram faulty movement patterns or desensitize an overactive nervous system.
The fear-avoidance cycle
Movement hurts, so you stop moving altogether. But total rest is actually a toxic prescription for musculoskeletal issues. This behavioral retreat triggers rapid muscle atrophy and joint stiffness, which explains why the subsequent attempt at activity feels even more excruciating. Breaking this vicious loop requires a conceptual shift. We must accept that discomfort does not automatically equal structural damage. Because the brain amplifies threat signals during periods of prolonged isolation, dodging physical activity ironically lowers your overall tolerance threshold.
Misunderstanding psychological modulation
Suggesting a mental health component to physical suffering often insults patients. They hear, It is all in your head. Let's be clear: neural pathways carrying nociceptive data directly intersect with emotional processing centers like the amygdala. Ignoring cognitive behavioral strategies means you are fighting a biological battle with one hand tied behind your back. It is not about wishing the agony away through positive vibes, yet thousands of individuals discard psychological tools due to misplaced pride.
The chronobiology factor: An expert perspective on timing
Aligning interventions with circadian rhythms
Most clinicians prescribe therapies based on convenient clock hours rather than biological reality. Your body does not operate on a static schedule. Inflammation markers typically peak during the early morning hours, which dictates a synchronized approach to implementing the 3 P's of pain relief. For instance, executing gentle physical stretching exactly when endogenous cortisol levels are naturally rising can drastically amplify the therapeutic window. Why do we ignore this internal clockwork when mapping out rehabilitation schedules?
Conversely, psychological unwinding exercises yield the highest neurological dividend when performed right before sleep. This strategic timing dampens the sympathetic nervous system, allowing the body to enter a restorative parasympathetic state. (Some pioneering clinics are finally tracking heart rate variability to customize these daily schedules). Optimizing the cadence of your interventions creates a compounding effect, transforming modest daily habits into a potent shield against systemic distress.
Frequently Asked Questions
Can you successfully manage severe neuropathic discomfort without pharmaceuticals?
Clinical data indicates that while 62% of patients with severe nerve damage achieve partial comfort through gabapentinoids, complete resolution almost always requires combining these drugs with physical desensitization protocols. Relying on chemical intervention alone leaves the underlying neural hypersensitivity untouched. Integrating targeted nerve-gliding exercises alongside cognitive behavioral pacing mechanisms yields a much higher success rate. As a result: a multimodal framework remains the gold standard for complex neurological cases.
How long does it take for psychological strategies to alter physical sensations?
Neuroimaging research demonstrates measurable alterations in gray matter density within the prefrontal cortex after just eight weeks of consistent mindfulness-based stress reduction practices. This structural remodeling directly correlates with a 30% reduction in subjective suffering scores among chronic back patients. The issue remains that patients expect instant rewiring, whereas neural plasticity demands sustained, daily engagement. In short, cognitive interventions function like physical training for your brain, requiring patience before the analgesic benefits manifest.
Is there a specific ratio between the physical and psychological components?
Every individual possesses a unique physiological profile, meaning there is no universal mathematical formula for balancing the three pillars of pain management. A patient recovering from an acute sports injury might require an 80/20 split heavily favoring physical rehabilitation and biomechanical adjustments. Meanwhile, a fibromyalgia sufferer dealing with central sensitization often finds greater success by dedicating 60% of their efforts to psychological grounding and stress modulation techniques. Dictating a rigid, one-size-fits-all percentage to a diverse patient population is a recipe for clinical failure.
A definitive paradigm shift in recovery
The current medical establishment remains obsessed with quick fixes, cutting out tissues or numbing nerves while ignoring the complete human experience. True healing demands that we stop viewing discomfort through a narrow, purely anatomical lens. By weaponizing the 3 P's of pain relief simultaneously, you regain control over an unruly nervous system instead of remaining a victim to it. This holistic approach requires active, uncomfortable effort rather than passive consumption. We must discard the outdated notion that a single silver bullet exists in a pharmacy bottle. Embrace the complexity of your biology, demand comprehensive care, and refuse to settle for superficial treatments that merely mask your symptoms.