The Anatomy of a Hidden Threat: What Is an Unruptured Brain Aneurysm Anyway?
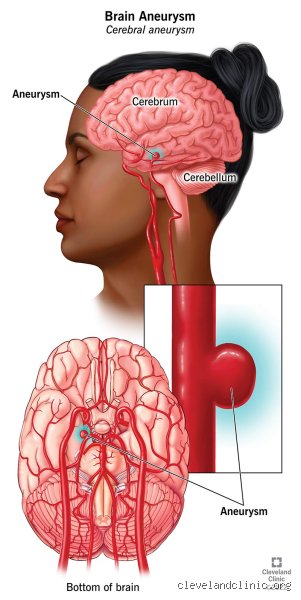
Picture a worn-out garden hose. Under high pressure, a weakened section of the rubber begins to balloon outward, thinning with every passing second. That is precisely what happens inside the cerebral vasculature. An unruptured brain aneurysm is a localized, abnormal ballooning of an artery wall within the brain that has not yet leaked or burst. Roughly 1 in 50 people in the United States is walking around with one right now, completely oblivious to its existence. Most of these vascular anomalies are found entirely by accident during routine MRIs for unrelated issues like chronic migraines or after minor concussions. I have seen patients completely upend their entire lives over a tiny, two-millimeter bulge that poses almost zero actual risk of rupture. It breaks my heart because the stress itself is often worse than the pathology.
The Silent Incidents and the Role of Hemodynamics
Where it gets tricky is understanding why they form in the first place. It is not just about weak tissue; it is a complex dance of fluid dynamics and biology. Blood flows through the Circle of Willis—the main arterial junction at the base of the brain—with immense, turbulent force. Over decades, this relentless pounding wears down the structural integrity of the vessel walls, specifically at branching points. And because these lesions rarely cause symptoms until they grow large enough to compress adjacent cranial nerves, they remain ghosts in the machine.
The Real Danger: Decoupling True Risk From Absolute Panic
People don't think about this enough, but finding an aneurysm does not mean you are handed a death sentence. The annual rupture rate for small, asymptomatic lesions is often less than 1% per year. Why then do we treat some immediately while leaving others completely alone? Because a rupture leads to a subarachnoid hemorrhage, a catastrophic type of stroke where blood floods the space surrounding the brain. It is a brutal reality, yet the medical establishment historically overcorrected by operating on every single bulge they encountered, frequently causing more harm through surgical complications than the natural history of the disease ever would have.
The Modern Decision Matrix: How Doctors Determine If You Need to Get Rid of It
Neurologists do not look at these anomalies in a vacuum. Instead, they rely heavily on landmark clinical data, specifically the Phase II International Study of Unruptured Intracranial Aneurysms (ISUIA) from 2003, which fundamentally altered how we calculate danger. When a specialist evaluates your brain, they are running a complex calculus based on size, morphology, and your personal medical history. Aneurysms measuring under 7 millimeters in the anterior circulation of the brain have an incredibly low statistical probability of ever causing trouble. But that changes everything if the lesion is located in the posterior circulation, such as the basilar artery, where even small bulges behave far more aggressively.
The PHASES Score and Your Personal Risk Profile
To standardize this guesswork, clinicians developed the PHASES score, an elegant predictive model that compiles data points including age, hypertension history, previous subarachnoid hemorrhage, aneurysm size, site, and geographic background. For instance, data shows that patients from Finland and Japan possess a significantly higher baseline risk of rupture for reasons that are still debated among geneticists. Are you a smoker? If so, your risk of a rupture skyrockets instantly. Nicotine actively degrades the structural matrix of the arterial wall, turning a stable vascular outpouching into an unstable, irregular nightmare.
When Shape Matters More Than Raw Size
A perfectly round, spherical sac is generally a peaceful tenant in your cranium. But what if it develops a secondary sac, commonly referred to as a daughter cyst? That irregular, lobulated geometry signals that the wall is structurally uneven and highly prone to failure. The issue remains that we cannot peer inside the living vessel wall to measure its exact tensile strength, meaning neurosurgeons must rely on these morphological red flags to make life-or-death recommendations.
Surgical Obliteration: The Direct Approaches to Eliminating the Bulge
If your medical team determines that the risk of waiting outweighs the risk of action, you enter the realm of active intervention. To get rid of an unruptured brain aneurysm, science offers two radically different pathways: open microsurgery and minimally invasive endovascular repair. The choice between them is a fierce battleground of anatomy, operator skill, and patient preference.
Microvascular Clipping: The Classic, Definitive Open-Brain Fix
This is the old-school, time-tested gold standard. Performed under general anesthesia, a neurosurgeon executes a craniotomy, carefully removing a small window of bone from the skull to access the brain. Utilizing ultra-high-powered surgical microscopes and delicate micro-instruments, the surgeon navigates through the natural clefts of the brain without disturbing the neural tissue itself. Once the compromised blood vessel is exposed, the surgeon places a tiny titanium clip—resembling a microscopic clothespin—permanently across the neck of the aneurysm.
This completely cuts off the blood supply, effectively killing the lesion on the spot. It is a brutal, exhausting procedure for the body, yet its long-term durability is unmatched. Once clipped successfully, the recurrence rate is practically zero. Except that you have to undergo a major brain operation to achieve that peace of mind, which explains why many patients balk at the prospect of open surgery when a less invasive alternative exists.
Endovascular Coiling: Navigating the Arterial Highway From Within
Welcome to the space age of interventional neuroradiology. Instead of cutting open the skull, a specialist makes a tiny puncture wound in your groin or wrist. They thread a long, flexible microcatheter through the femoral or radial artery, steering it all the way up through the aorta and into the delicate vessels of the neck and brain. Guided by continuous, real-time fluoroscopic X-ray imaging, the physician maneuvers the catheter tip directly into the empty dome of the aneurysm.
Then, they deploy dozens of microscopic platinum coils. These threads of metal bundle up inside the sac like a ball of yarn, slowing the blood flow to a crawl. This triggers a localized clotting cascade, thrombosing the lesion and blocking it off from the high-pressure arterial stream. It sounds perfect, right? But here is where the catch lies: coils can compact over time due to the relentless pounding of your pulse, occasionally requiring a follow-up procedure years down the road to pack in more metal.
Advanced Endovascular Innovations: Flow Diverters and Web Devices
Not every vascular defect is shaped like a neat little berry with a distinct neck. What happens when the entire side of an artery turns into a wide-necked, fusiform monstrosity? Traditional coiling would simply spill out into the parent artery, causing a massive, catastrophic stroke. For these complex structural dilemmas, the medical device industry engineered flow-diverting stents, such as the Pipeline Embolization Device, which revolutionized neuro-intervention in the early 2010s.
Re-engineering the Bloodroad With Flow Diversion
Instead of packing the bulge itself, the operator deploys a densely woven mesh cylinder right across the opening of the aneurysm inside the main blood vessel. Think of it as a bypass wall. The mesh allows blood to continue down the main highway but severely restricts its ability to swirl into the weakened pouch. Deprived of high-velocity inflow, the blood stagnant inside the aneurysm clots off, and over the course of several months, the body actually grows a brand-new, healthy layer of endothelial cells right over the mesh stent. It literally remodels the inside of your brain's plumbing. We're far from the crude tools of the 1980s; this is pure bio-engineering.