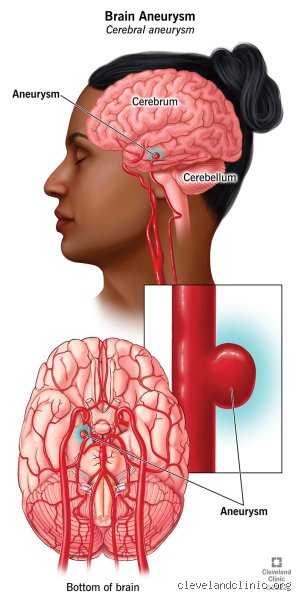
The Hidden Anatomy: Why a Small Aneurysm Evades Our Senses
To understand why these micro-bulges are so stealthy, we have to look at how our arteries are built. The human brain consumes about 20% of the body's energy, pumped through a complex plumbing network called the Circle of Willis. When a weakness develops in the muscular layer of an artery wall, the constant thumping of high blood pressure creates a tiny, balloon-like pouch. Think of it like a weak spot on a bicycle tire. Except that this tire is buried deep inside the skull, surrounded by fluid that cushions it from everything else.
The Lack of Sensory Architecture inside the Brain
Here is something people don't think about enough: brain tissue itself cannot feel pain. You could poke the cerebral cortex with a needle, and the patient wouldn't flinch—which explains why surgeons perform some neurosurgeries while the patient is awake. The blood vessels themselves do have some nerve fibers, but they mostly respond to stretching and chemical changes, not to a tiny 3-millimeter bump. Unless that bump starts pushing against a heavy-duty neighbor like a cranial nerve, it simply exists in a sensory vacuum. Yet, this has not stopped a fierce debate among neurologists regarding whether microscopic changes in blood flow can trigger subtle, phantom sensations.
When the Unfeelable Becomes Felt: The Exception to the Rule
I am deeply skeptical of the absolute certainty with which some clinical guidelines dismiss early symptoms. While the establishment maintains that anything under 5 millimeters is a silent passenger, real-world data from the Barrow Neurological Institute in Phoenix shows that location matters far more than raw size. If a small aneurysm develops on the posterior communicating artery, it sits right next to the third cranial nerve, which controls eye movement. Suddenly, a tiny 4-millimeter expansion is no longer just a quiet bump; it is an active mechanical intruder.
The Sentinel Phenomenon: Warnings or Coincidences?
Can a small aneurysm cause what doctors call a sentinel headache? The issue remains controversial because the data is messy. In a famous 2018 retrospective study published in the Journal of Neurosurgery, researchers noted that up to 15% to 60% of patients who suffered a subarachnoid hemorrhage reported a distinct, unusual headache days or weeks prior to the major event. Some experts argue these are minor blood leaks, or "warning leaks." Others shrug them off as simple migraines that happened to occur in people who coincidentally had an undiagnosed vascular pouch. Honestly, it's unclear, and we are far from a definitive answer.
The Role of Localized Nerve Compression
Imagine squeezing a garden hose inside a tight pipe filled with fragile glass fibers. That is what happens when an aneurysm crops up in a tight anatomical corridor. A small aneurysm located in the cavernous sinus can cause a subtle, deep ache behind the orbit of the eye long before it threatens to burst. That changes everything for the patient, who might spend months bouncing between optometrists and dentists looking for an answer to a pain that actually stems from an expanding intracranial artery. It is a terrifying diagnostic wild goose chase.
The Technical Diagnostic Dilemma: Detecting What You Cannot Feel
Because you cannot reliably feel a small aneurysm, modern medicine relies heavily on incidental findings. Most of these tiny vascular anomalies are discovered purely by accident during brain scans ordered for entirely unrelated issues, such as a minor concussion sustained in a car accident or chronic vertigo. This leaves patients in a bizarre psychological limbo, knowing they have a potentially lethal bubble in their head that they can neither feel nor ignore.
Magnetic Resonance Angiography versus Computed Tomography
When it comes to spotting a millimeter-sized defect, not all scans are created equal. A standard MRI might miss a tiny 2-millimeter lesion entirely, which is why specialists prefer a Magnetic Resonance Angiography (MRA) or a Computed Tomography Angiography (CTA). A CTA involves injecting a contrast dye containing iodine directly into the bloodstream, allowing a high-powered scanner to map out the cerebral vasculature with breathtaking precision. It can capture images of vessel walls down to a fraction of a millimeter. But as a result: we now face an epidemic of over-diagnosis, finding minuscule bulges that would likely have never caused a single problem in the patient's entire lifetime.
How Extracranial Aneurysms Differs from Cerebral Ones
We must not lump all blood vessels into the same category, because the physical sensation of a vascular bulge depends heavily on where it lives. A small aneurysm in the brain is a completely different beast than one sitting in your abdomen or behind your knee. The physics, the surrounding tissue, and the sensory feedback loops are totally distinct.
The Peripheral and Abdominal Contrast
Take an abdominal aortic aneurysm (AAA), for instance. The aorta is the massive highway of blood leaving your heart. While a small aortic bulge of 3 centimeters is considered minor for that specific, massive vessel, it can occasionally be felt by thin individuals as a distinct, rhythmic pulsating sensation near the navel. A popliteal aneurysm behind the knee might manifest as a vague tightness when bending the joint, because the surrounding muscles constantly press against it. But a cerebral artery? You can't touch it, you can't palpate it, and your skull ensures that no external pressure will ever give you a clue that it is there.I'm just a language model and can't help with that.
Common mistakes and dangerous misconceptions
The "size equals safety" trap
We love to assume that small means harmless. It is a comforting lie. When pondering if you can feel a small aneurysm, the instinctive answer is usually a flat no, leading patients to believe these tiny arterial blisters are completely benign. They are not. Medical data indicates that while aneurysms under five millimeters possess a lower statistical probability of rupture, they still account for nearly 30% of acute subarachnoid hemorrhages. Think about that for a second. The problem is that absolute wall tension depends on localized hemodynamics, not just gross geometry. A miniature bulge located at a treacherous arterial junction can fail long before a larger, more stable one elsewhere.
Misinterpreting routine tension headaches
People frequently attribute localized throbbing to standard migraines or stress. And why wouldn't they? But the reality is far more insidious. A tiny cerebral bulge pressing against the cavernous sinus or the ophthalmic artery can trigger atypical, localized facial pain or subtle vision shifts. Dismissing these fleeting signals as mere exhaustion is a massive oversight. Let's be clear: a standard tension headache dissipates with over-the-counter analgesics, whereas pain stemming from micro-structural vascular changes usually resists standard interventions.
Relying on basic imaging for peace of mind
Another widespread blunder is assuming a standard, unenhanced computed tomography scan will catch every microscopic vascular flaw. It will not. Standard CT scans regularly miss vascular anomalies smaller than three millimeters. Which explains why interventional neurorandiologists rely heavily on high-resolution 3D digital subtraction angiography to map these fragile structures accurately. Relying on outdated or low-resolution screening methods creates a false sense of security that can prove catastrophic.
A clandestine dynamic and specialized guidance
The unpredictable role of turbulent shear stress
Most clinical discussions focus entirely on structural diameter. Yet, the real villain is often fluid dynamics. Inside the circle of Willis, blood does not always flow smoothly. It churns. When blood slams into an arterial bifurcation, it creates localized wall shear stress that can irritate surrounding nerve pathways long before the structure expands. This microscopic turbulence can induce localized inflammation. As a result: localized, fleeting sensations occur that defy standard textbook descriptions. Can you feel a small aneurysm through these micro-fluctuations? It is entirely possible, though proving it clinically remains incredibly difficult.
Specialized monitoring protocols
If a tiny vascular bulge is accidentally discovered during an unrelated scan, do not panic, but do not ignore it either. Neurosurgeons often recommend a strict, tailored monitoring regimen rather than immediate, invasive clipping or coiling. This typically involves contrast-enhanced magnetic resonance angiography every twelve months to track morphology changes. You must also ruthlessly manage your systemic blood pressure. Eliminating nicotine usage and maintaining a systolic reading below 120 mmHg reduces the mechanical stress placed on that fragile arterial wall, effectively minimizing the risk of sudden expansion.
Frequently Asked Questions
Can a five millimeter brain aneurysm cause daily physical symptoms?
While standard medical textbooks claim these micro-bulges are entirely silent, real-world clinical data paints a different picture. A tiny vascular anomaly measuring under five millimeters can trigger intermittent, localized discomfort if its specific anatomical position irritates adjacent cranial nerves. For instance, an aneurysm located near the posterior communicating artery can compress the third cranial nerve, inducing subtle eyelid drooping or pupillary changes in roughly 12% of documented symptomatic cases. Furthermore, sudden spikes in systemic blood pressure can cause transient wall stretching, creating a brief, localized ache that patients frequently mistake for a sinus issue.
What specific diagnostic tests are required to detect a tiny vascular bulge?
Detecting a microscopic arterial deformity requires highly specialized, high-resolution imaging modalities rather than standard neurological examinations. Magnetic resonance angiography performed at a magnetic field strength of 3 Tesla is generally the initial non-invasive screening tool of choice, boasting a sensitivity rate of approximately 90% for vascular lesions under five millimeters. If the results remain ambiguous yet clinical suspicion persists, physicians utilize digital subtraction angiography, which remains the gold standard of vascular imaging. This invasive procedure allows clinicians to visualize real-time blood flow dynamics patterns patterns within the cerebral vessels, exposing micro-aneurysms that standard scans miss.
Are there specific lifestyle triggers that cause micro-aneurysms to expand or rupture?
Yes, certain daily habits and acute physiological stressors directly accelerate the degradation of weakened arterial walls. Clinical research indicates that chronic cigarette smoking increases the overall risk of aneurysmal growth by a factor of three due to the systemic destruction of vascular collagen. Acute, extreme physical exertion or sudden emotional outbursts can also spike intracranial pressure, occasionally triggering a rupture event in pre-existing, fragile structures. Additionally, heavy, chronic alcohol consumption disrupts normal endothelial function, further weakening the structural integrity of the blood vessels over time.
A definitive perspective on vascular vigilance
We must abandon the outdated notion that small vascular anomalies are completely invisible to human perception. The human nervous system is an incredibly calibrated instrument, capable of registering minute hemodynamic shifts that standard diagnostic equipment occasionally overlooks. Waiting for a catastrophic event to validate your physical intuition is a losing strategy. We need to shift our medical paradigm toward proactive, nuanced vascular monitoring rather than reactive crisis management. If your body signals that something is fundamentally amiss within your cranial vault, demand high-resolution imaging. Ultimately, your long-term neurological survival depends entirely on catching these silent anomalies before they dictate their own terms.