Beyond the Average: Defining Longevity and the Demographics of Early Mortality
We treat life expectancy like a fixed prophecy, a ticking biological clock set at birth. The truth is much messier. Demographers use period life expectancy, which is essentially a snapshot of a specific year's death rates applied to a hypothetical generation. It is a useful tool, except that it wildly skews reality when a crisis hits. If a country suffers a spike in infant mortality, the average plunging downward does not mean every adult suddenly dies at fifty. It means the starting line is a minefield.
The Statistical Trap of Infant Mortality Rates
Where it gets tricky is separating historical baggage from current health crises. When we ask what group of people has the shortest life expectancy, the data is heavily weighed down by children who never make it to their fifth birthday. If you survive childhood in a high-mortality zone, your chances of reaching sixty or seventy shoot up dramatically. Because of this mathematical quirk, a single statistic can mask the resilience of older populations while highlighting a catastrophic failure in neonatal care.
How Conflict and Geography Warp the Numbers
Look at the Central African Republic or Lesotho. It is easy to blame a single factor, but the issue remains an intricate web of geography, unstable governance, and lack of infrastructure. In these regions, a simple infection becomes a death sentence. And honestly, it is unclear whether international aid models even grasp how to fix these localized collapses without making dependencies worse.
The Deadliest Coordinates: Geopolitical Zones Where Life is Cut Short
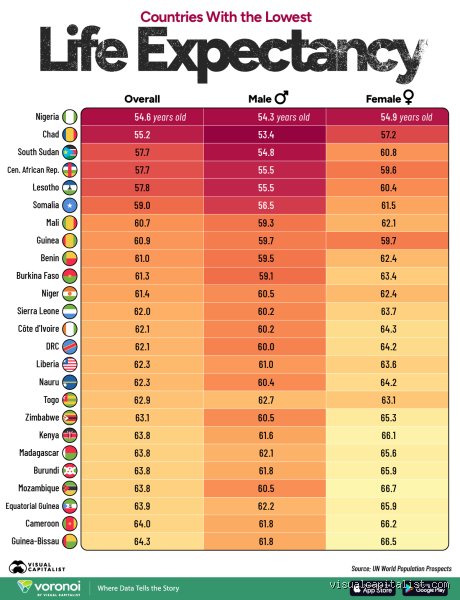
If you want to understand premature death, you have to look at Sub-Saharan Africa and pockets of Eastern Europe. The gap between the longest-living populations—like women in Japan who routinely breeze past 87—and the shortest is a staggering thirty-five years. That changes everything about how we view human progress. We are far from a unified global standard of health.
The Central African Republic and the 53-Year Ceiling
In the Central African Republic, decades of civil unrest, coupled with a total collapse of the healthcare apparatus, have cemented its place at the bottom of global longevity rankings. A child born in Bangui in 2024 faces odds that look closer to medieval Europe than the 21st century. Malaria, malnutrition, and HIV form a lethal triad here. Yet, Western analysts often talk about these numbers as if they are inevitable consequences of tropical climates rather than direct results of political destabilization and resource exploitation.
Lesotho and the Heavy Toll of the HIV Epidemic
Then there is Lesotho, a landlocked kingdom entirely surrounded by South Africa. Here, the story shifts. It is not just about active war zones; it is about an insidious health crisis. The adult HIV prevalence rate in Lesotho has historically hovered around 20%, one of the highest in the world. Imagine a society where a fifth of the productive workforce is fighting a chronic, stigmatized virus. Consequently, the life expectancy for men in Lesotho dropped to around 50 years in the late 2010s, though aggressive antiretroviral rollouts have triggered a fragile rebound lately.
The Intersection of Gender and Hardship: Why Men Die Sooner Worldwide
Across almost every single demographic group, men die younger than women. It is a biological and behavioral constant. Even in the most impoverished nations, the male subset of the population consistently claims the title of the group with the shortest life expectancy. Why? Biological vulnerability plays a part, but behavioral risks and societal expectations do the heavy lifting.
Biological Disadvantages Versus Risk-Taking Behavior
Men are built differently, and not always to their benefit. Estrogen offers women a degree of cardiovascular protection that men simply lack until later in life. But nature only accounts for a fraction of the gap. The real killer is what happens when you mix biology with culture. Men are far more likely to engage in heavy alcohol consumption, smoke tobacco, and work in high-risk industries like mining or subsistence farming in volatile regions. In Russia, for instance, a massive ten-year gender gap exists, driven largely by cardiovascular disease and alcohol-related accidents among working-class men.
The Cultural Avoidance of Healthcare
People don't think about this enough: men are notoriously terrible at going to the doctor. This is not just an American or European phenomenon; it is a global pattern. In patriarchal societies, admitting illness is often viewed as a sign of weakness, which explains why men frequently present with advanced, untreatable stages of chronic conditions. By the time a clinic visit becomes unavoidable, the window for effective intervention has closed completely.
Comparing Global Hardship: Indigenous Populations in Wealthy Nations
To truly understand how this works, we must look past national averages. You do not need to travel to a developing nation to find shocking mortality disparities. Sometimes, the group with the shortest life expectancy lives right inside the borders of the world’s wealthiest empires.
The Disparity Within Australia and North America
Consider the Indigenous populations of Australia, Canada, and the United States. In Australia, Aboriginal and Torres Strait Islander men have a life expectancy that is roughly 8.6 years shorter than non-Indigenous Australians. Why does a First Nations man in a wealthy nation like Australia face a longevity profile similar to someone living in a developing economy? The answers lie in systemic marginalization, higher rates of chronic diseases like diabetes, and historical trauma that echoes through generations. This reality shatters the comfortable illusion that high national GDP automatically guarantees a long life for everyone inside the border.
Common mistakes and misconceptions when assessing global longevity
The trap of the statistical average
When you read that a specific demographic has the shortest life expectancy, your brain instantly imagines individuals dropping dead at age thirty. But let's be clear: this is a mathematical illusion. High infant mortality historically skewed these numbers into oblivion, dragging down the statistical mean while adults still lived to grey-haired seniority. If a community suffers a devastating under-five mortality rate, the overall metric plummets, yet the survivors might regularly cross the seventy-year threshold. Confounding life expectancy at birth with lifespan remains the most ubiquitous error in public health reporting.
The genetic determinism myth
Why do we stubbornly blame DNA for systemic failures? It is incredibly easy to look at marginalized populations, such as indigenous communities in isolated regions, and assume their truncated survival rates stem from a biological predisposition to disease. Except that genetic variations account for a minuscule fraction of these differences compared to the crushing weight of the social determinants of health. Epigenetics shows us that environment alters gene expression, which explains why poverty and chronic discrimination literally accelerate cellular aging, masquerading as inherited traits when they are actually societal constructs.
Ignoring the volatility of war-torn zones
We often treat longevity data as static, unchanging realities written in stone. Yet, the group of people has the shortest life expectancy can shift in a matter of months when geopolitical stability collapses. During the height of the Syrian conflict or during localized famines in the Horn of Africa, the demographic math recalibrated violently, demonstrating that conflict-induced mortality spikes skew data dramatically. You cannot analyze long-term biological trends without accounting for these temporary, acute geopolitical catastrophes that rewrite regional survival statistics overnight.
The spatial mismatch: Hidden pockets of mortality
The tragedy of rural healthcare deserts
There is a little-known geographic phenomenon that experts call spatial mismatch, where the people who need medical intervention the most live the furthest from it. If you examine deep pockets of the Appalachian region in the United States or remote parts of the Australian Outback, you find life expectancies that rival war zones. The issue remains that building a state-of-the-art oncology ward or a trauma center in a county with fewer than ten thousand residents is financially unviable for corporate healthcare systems. As a result: individuals residing in these geographic dead zones face a ticking clock, where a simple cardiovascular event becomes a death sentence due to a ninety-minute ambulance ride. (It makes you wonder if our map-making skills have outpaced our human empathy.) This brings us to a stark realization: the group of people has the shortest life expectancy is frequently defined not by national borders, but by postal codes.
Frequently Asked Questions
Which country currently records the absolute lowest life expectancy at birth?
According to recent United Nations demographic assessments, the Central African Republic routinely registers the lowest national figures, hovering around fifty-four years for the general population. This grim reality is compounded by systemic malnutrition, ongoing civil instability, and a severe shortage of trained medical personnel. Because of these overlapping crises, infectious diseases like malaria and tuberculosis ravage communities that lack basic sanitation infrastructure. In short, the nation faces a structural deficit where high maternal mortality rates combine with endemic violence to suppress the statistical average far below the global standard.
How does substance abuse impact the longevity of specific subgroups?
The devastating rise of synthetic opioids has rewritten the demographic landscape across portions of North America, particularly among working-class males aged twenty-five to forty-four. This specific demographic has experienced a measurable retraction in survival metrics over the past decade, a phenomenon economists describe as deaths of despair. Alcoholism and liver disease similarly decimate isolated northern indigenous groups where economic opportunities have completely vanished. But are we willing to look past the symptoms to address the root psychological trauma? The problem is that treating addiction as a moral failing ignores the macroeconomic collapse that precipitates these public health emergencies in the first place.
Can economic migration improve the life expectancy of vulnerable populations?
The relationship between migration and longevity is highly paradoxical, often referred to by sociologists as the healthy migrant effect. Individuals who possess the physical and financial stamina to migrate from low-resource nations to wealthy states often outlive their native-born peers initially. However, this advantage erodes over time as the immigrants adopt western diets and face the chronic stress of systemic socioeconomic marginalization. Statistics indicate that within two generations, the longevity metrics of migrant descendants typically assimilate downward, matching the socioeconomically disadvantaged groups within their host countries.
A definitive verdict on structural survival
We must stop treating shortened lifespans as an unfortunate byproduct of geography or fate. Let's be clear: the group of people has the shortest life expectancy is always the one intentionally starved of political capital and economic agency. Whether we are discussing the victims of systemic racism in wealthy urban centers or forgotten rural populations in developing nations, the fundamental culprit is never a lack of medical knowledge. The issue remains a profound, global distribution crisis of resources and human empathy. We possess the tools, the wealth, and the technology to equalize global survival metrics, yet we choose to tolerate a world where poverty dictates the day you die. It is time to abandon comfortable statistical detachments and aggressively fund universal healthcare infrastructure as an absolute moral imperative.