The Deceptive Mimic: What We Are Actually Dealing With in the Clinic
Autoimmune pancreatitis is a distinct, immune-mediated form of chronic pancreatitis characterized by a prominent fibroinflammatory infiltrate. The thing is, this pathology comes in two entirely different flavors that clinicians frequently lump together, creating massive confusion. Type 1 AIP is the pancreatic manifestation of IgG4-related disease, an systemic systemic syndrome that tends to strike older men and happily wreaks havoc on multiple organs simultaneously. Then you have Type 2, which is an entirely different beast altogether, showing no systemic links, normal IgG4 levels, and a bizarrely strong association with inflammatory bowel disease, particularly ulcerative colitis. Why does this distinction matter so much? Because when you are sitting in a multidisciplinary team meeting looking at a swollen pancreatic head, you are trying to avoid sending someone to a massive, life-altering Whipple surgery that they might not even need.
A Histological Tale of Two Distinct Diseases
Let us look closely at what is happening beneath the microscope. Type 1 is defined by lymphoplasmacytic sclerosing pancreatitis, a distinct pattern featuring storiform fibrosis, obliterative phlebitis, and an abundance of IgG4-positive plasma cells. Type 2, conversely, features granulocyte-epithelial lesions where neutrophils actively destroy the ductal epithelium. Honestly, it is unclear why the immune system chooses these two radically different pathways to attack the exact same organ. It is a medical mystery that keeps pathologists arguing during grand rounds, but for the treating physician, it means your diagnostic strategy must be incredibly nimble.
Cracking the ICDC Code: Imaging, Serology, and the Burden of Proof
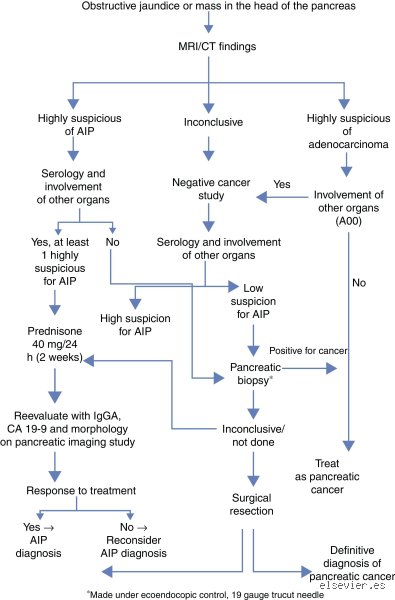
How do we actually go about ruling out this disease when a patient presents with painless obstructive jaundice? The international community realized that relying on a single test was a recipe for disaster, hence the creation of the International Consensus Diagnostic Criteria in 2011. This framework evaluates five core dimensions: parenchymal imaging, ductal imaging, serology, other organ involvement, and histology. But here is where it gets tricky. You can have a patient who meets the imaging criteria perfectly, yet their serology is completely normal, which happens in up to thirty percent of confirmed Type 1 cases. Does a normal IgG4 titer mean you can safely cross the disease off your list? We are far from it, and assuming so is a rookie mistake that can delay proper management.
The Radiologist's Lens: Looking for the Sausage sign
Standard computed tomography or magnetic resonance imaging remains your first line of defense, but the findings require a highly trained eye. On a contrast-enhanced CT scan taken during the pancreatic phase, classic autoimmune pancreatitis manifests as diffuse enlargement of the gland, turning the normal feathered architecture into a smooth, featureless mass often referred to as a sausage-like appearance. A low-attenuation capsule-like rim surrounding the pancreas is a highly specific signature of Type 1 disease, reflecting peripancreatic fluid and inflammatory fibrotic tissue. Yet, except that sometimes the disease decides to be focal rather than diffuse. When a focal mass occurs in the pancreatic head, it mimics a malignant tumor perfectly, causing a segment of upstream main pancreatic duct dilation that makes every radiologist's stomach drop. Magnetic resonance cholangiopancreatography will often show long, multi-segment strictures without the marked upstream dilation typically seen in carcinomas, a subtle clue that changes everything.
The Serological Trap: Understanding the True Limits of IgG4 Testing
Blood work seems like an easy out, but serology is a double-edged sword in this arena. The standard diagnostic threshold is a two-fold elevation of serum IgG4, typically meaning values above 280 milligrams per deciliter. And yet, life is rarely that simple. Did you know that up to ten percent of patients with pancreatic cancer also present with elevated IgG4 levels? If you rely solely on a mild serological elevation to diagnose autoimmune pancreatitis, you might accidentally watch a resectable tumor progress to stage four while you blissfully prescribe useless immunosuppressants. That is a terrifying prospect, which explains why we look for other organ involvement, such as sialadenitis, retroperitoneal fibrosis, or IgG4-related sclerosing cholangitis, to tip the scales toward a systemic autoimmune process.
The Invasive Frontier: Histology and Response to Steroid Trials
When imaging and blood tests leave you stranded in a diagnostic gray zone, you have to go in and get tissue. Endoscopic ultrasound-guided fine-needle biopsy has largely supplanted older fine-needle aspiration techniques because cytology alone cannot show you the architecture of storiform fibrosis or obliterative phlebitis. You need core tissue pieces, ideally obtained with twenty-two or twenty-five gauge biopsy needles, to see the required greater than ten IgG4-positive cells per high-power field. People don't think about this enough, but a negative biopsy never truly rules out cancer; it just means you didn't hit the malignant cells with your needle. It is an uncomfortable reality that every gastroenterologist must accept.
The Controversial Steroid Trial: A Diagnostic Tool or a Dangerous Gamble?
The ICDC allows for a diagnostic response to a steroid trial, typically using oral prednisolone at a dose of forty milligrams per day for exactly two weeks. Genuine autoimmune pancreatitis responds dramatically, with a rapid resolution of mass lesions and a significant drop in IgG4 levels. But what if the mass is actually a cancer that happens to have a lot of surrounding inflammatory reaction? A slight, transient reduction in tumor-associated edema can fool an optimistic clinician into thinking they have won, while the underlying malignancy continues to replicate. As a result, a steroid trial should absolutely never be attempted unless a thorough workup, including EUS-FNB, has failed to find malignancy, and even then, follow-up imaging at the fourteen-day mark is mandatory to prove unequivocal regression.
Differentiating the Alternatives: Autoimmune Pancreatitis vs. Pancreatic Adenocarcinoma
The core clinical dilemma is separating autoimmune pancreatitis from pancreatic ductal adenocarcinoma, a disease with a brutal five-year survival rate of roughly thirteen percent. How do we draw the line when both present with weight loss, jaundice, and a pancreatic mass? Let us break down the critical differences that can save a life.
First, look at the patient's age and clinical presentation. While cancer patients often present with profound cachexia and unrelenting back pain, AIP patients are more likely to have fluctuating jaundice and milder constitutional symptoms. Furthermore, the tumor marker CA 19-9 is usually wildly elevated in adenocarcinoma, whereas in AIP it is either normal or only moderately elevated due to biliary obstruction. The table below illustrates the contrasting features that clinicians must weigh during evaluation.
| Diagnostic Feature | Autoimmune Pancreatitis (Type 1) | Pancreatic Ductal Adenocarcinoma |
| Gland Morphology | Diffuse sausage-like enlargement or focal mass with capsule-like halo | Hypodense, poorly defined focal mass with irregular borders |
| Main Pancreatic Duct | Multiple, long strictures involving more than one-third of the duct length | Abrupt cutoff with marked upstream dilation (double duct sign) |
| Serum IgG4 Levels | Elevated, frequently greater than two times the upper limit of normal | Usually normal, though mildly elevated in up to 10% of cases |
| Other Organ Involvement | Common (biliary strictures, salivary glands, retroperitoneum) | Absent (except for direct metastatic disease to liver or lungs) |
The issue remains that these criteria are guidelines, not absolute laws written in stone. I have seen cases where a focal AIP mass caused a classic double duct sign, completely mimicking a tumor in the head of the pancreas. What do you do when the data points contradict one another? You keep digging, because the alternative is rushing a patient into a major resection or, conversely, letting a fast-growing cancer slip away under a cloud of steroids.
Common Pitfalls and Misconceptions in the Diagnostic Process
The IgG4 Obsession
Clinicians frequently fall into the trap of treating elevated serum IgG4 levels as an absolute verdict. The problem is that up to 5% of the healthy population and nearly 10% of patients with conventional pancreatic adenocarcinoma also exhibit elevated titers of this biomarker. Relying solely on a blood draw to rule out autoimmune pancreatitis invites catastrophic misdiagnosis. You cannot simply check a box because the laboratory report returns a value above 140 mg/dL. Conversely, Type 2 autoimmune pancreatitis leaves absolutely no serological footprint, completely evading IgG4 detection. If you stop hunting because the serology is normal, you will miss the disease entirely.
Biopsy Blunders
Another major stumble involves misinterpreting core needle biopsies versus fine-needle aspirations. Cytology specimens obtained via standard endoscopic ultrasound often yield nothing but generic inflammatory debris, which explains why so many pathologists hesitate to commit to a diagnosis. To definitively identify lymphoplasmacytic sclerosing pancreatitis, you must obtain core tissue samples showing storiform fibrosis and obliterative phlebitis. But how often does a hurried endosonographer change needles mid-procedure? Not nearly enough, unfortunately. A negative cytology smear never allows you to rule out autoimmune pancreatitis safely; it merely confirms you sampled a non-specific zone of inflammation.
The Steroid Trial: An Expert Double-Edged Sword
The Dangerous Illusion of Remission
Initiating a response assessment with oral corticosteroids remains a classic diagnostic maneuver, yet it conceals a perilous diagnostic trap. Let's be clear: pancreatic cancer can transiently shrink and show metabolic improvement under the influence of strong anti-inflammatory agents. If a clinician witnesses a 30% reduction in a pancreatic mass after two weeks of prednisone, they might prematurely celebrate and permanently rule out pancreatic cancer in favor of an autoimmune etiology. This brief honeymoon period delays oncological surgery, often with fatal consequences. Why do we still treat steroid responsiveness as a definitive proof of benign disease when malignant stromal reactions can also temporarily quiet down?
The Strict Two-Week Horizon
True experts utilize the steroid trial with extreme discipline, maintaining a zero-tolerance policy for ambiguous results. Imaging must be repeated precisely 14 days after starting a regimen of 0.6 mg/kg daily. If the radiological manifestations do not show near-complete resolution, the autoimmune hypothesis should be discarded immediately. Because waiting any longer allows an aggressive adenocarcinoma to metastasize under the guise of an organizing mass, you must pivot to surgical resection without hesitation. (We must admit our clinical diagnostic algorithms are only as good as the clinician's willingness to admit they might be wrong.)
Frequently Asked Questions
Can a normal serum IgG4 level completely rule out autoimmune pancreatitis?
No, a completely normal serological profile is entirely insufficient to exclude this condition from your differential diagnosis. Statistical data indicates that approximately 30% of patients diagnosed with biopsy-proven Type 1 AIP present with completely normal IgG4 concentrations throughout their entire disease course. Furthermore, Type 2 AIP, which accounts for nearly 15% of all global cases, is characterized by a total absence of elevated serum IgG4 markers. Diagnostic protocols must therefore synthesize histopathology and cross-sectional imaging features rather than relying on a solitary laboratory test. As a result: an isolated blood test remains a notoriously weak diagnostic shield against misclassification.
How does the presence of other autoimmune conditions affect the diagnostic evaluation?
The presence of extra-pancreatic manifestations dramatically alters the diagnostic probability matrix but never provides a shortcut around a rigorous workup. Approximately 40% of patients afflicted with Type 1 AIP exhibit concurrent conditions such as IgG4-related sclerosing cholangitis, retroperitoneal fibrosis, or salivary gland swelling. Conversely, Type 2 AIP displays a strong, unique epidemiological association with inflammatory bowel disease, particularly ulcerative colitis, which is present in up to 30% of these specific cases. The issue remains that a patient with confirmed ulcerative colitis can still independently develop an aggressive pancreatic malignancy. Therefore, while background autoimmunity guides clinical suspicion, it never yields enough diagnostic leverage to bypass mandatory tissue acquisition or advanced parenchymal imaging.
What specific radiologic features help differentiate autoimmune pancreatitis from pancreatic cancer?
Classic cross-sectional imaging reveals a diffusely enlarged, sausage-shaped pancreas accompanied by a distinct, low-attenuation capsule-like rim in roughly 50% of AIP presentations. Unlike conventional pancreatic adenocarcinoma, which typically induces abrupt cutoff of the main pancreatic duct with severe upstream parenchymal atrophy, AIP typically manifests as a long, non-dilated, multi-focal stricture. Medical literature confirms that a ductal cutoff greater than 2 millimeters or severe upstream dilation exceeding 5 millimeters strongly points toward a malignant process rather than an autoimmune phenomenon. Except that atypical, focal variants of AIP mimic tumors so perfectly on computed tomography that even seasoned radiologists misclassify them in 15% of initial interpretations. Consequently, you must combine these specific ductal metrics with positron emission tomography or endoscopic ultrasound to achieve acceptable diagnostic clarity.
An Uncompromising Synthesis for the Modern Clinician
Diagnosing pancreatic pathologies demands a rejection of clinical complacency and a total abandonment of diagnostic shortcuts. We cannot continue to treat the differentiation between a treatable benign condition and a lethal malignancy as a casual academic exercise. The current medical landscape tolerates far too much ambiguity, often leading to unnecessary whipple procedures or, worse, delayed cancer care. It is time to enforce rigid, time-delimited diagnostic protocols where tissue acquisition reigns supreme over fickle blood tests. In short, your default operational stance must always favor a malignant diagnosis until comprehensive, multi-modal evidence proves otherwise. Only through disciplined diagnostic skepticism can we protect patients from the devastating consequences of a misdiagnosed pancreatic mass.