The Messy Reality of Defining the Best Age to Get Your Tubes Tied
We need to talk about the CREST study. Conducted by the Centers for Disease Control and Prevention, this landmark piece of research tracked women for fourteen years after their sterilization procedures. What they found flipped the clinical world upside down, revealing that twenty-three percent of women sterilized before age thirty experienced profound regret later in life. Conversely, for those who underwent the knife after turning thirty, that number plummeted to just under six percent. Where it gets tricky is translating these dry statistics into actual human lives.
A Medical System Stuck in the Past
Go into any suburban clinic in Ohio or a major hospital in Boston, and the story is identical. A twenty-four-year-old woman requests a tubal ligation, only to be told she might meet the man of her dreams tomorrow and change her mind. I find this paternalistic gatekeeping absolutely infuriating because it treats grown women like capricious children. Yet, physicians are terrified of lawsuits, which explains why many self-impose an informal rule requiring patients to be at least twenty-five, or even thirty, before they will even book the operating room. Is it fair? Absolutely not. But that changes everything when you are trying to navigate the healthcare system today.
The Statistical Cliff of Regret
Age is a proxy for life experience, not wisdom. The issue remains that our twenties are a chaotic blur of identity shifting, career building, and relationship churning. Data from the American College of Obstetricians and Gynecologists (ACOG) suggests that the single greatest risk factor for post-sterilization regret is not actually how many kids you have, but how young you were on the day of the surgery. If you sign those consent forms at twenty-one, you are statistically swimming upstream against your future self. People don't think about this enough when they are locked in the heat of a temporary lifestyle choice.
The Biological and Legal Gauntlet of Your Twenties
And then there is the paperwork. Federal Medicaid regulations in the United States enforce a strict twenty-one-year-old age minimum and an mandatory thirty-day waiting period for sterilization, meaning if you are twenty and broke, the government effectively decides your reproductive future for you. Private insurance might play by different rules, but the cultural barriers remain identical.
Why Youth Invites Medical Gaslighting
Imagine sitting across from a surgeon who refuses to look at your spreadsheets detailing your financial choices and instead smiles condescendingly while muttering about your future husband. It happens every single day. Doctors look at a twenty-two-year-old and see a walking ball of hormonal transition, disregarding the fact that nulliparous women—those who have never given birth—often possess the most unwavering desire to remain childfree forever. The friction is exhausting. Because of this, the best age to get your tubes tied often becomes the age at which a doctor will finally stop patronizing you and actually hand you the scalpel.
The Nulliparous Paradox
Here is a weird anomaly that traditional medicine hates to acknowledge: women who have already had three kids by age twenty-four are actually more likely to regret getting their tubes tied than a twenty-four-year-old who has never had a single child. Why? Because the young mother’s life is still tied to the volatile landscape of early relationships, whereas the intentionally childfree woman has usually contemplated her stance since puberty. Yet, who gets approved faster by the hospital board? The mother of three, every single time. We are far from achieving a system based on actual logic.
The Golden Zone: Why Thirtysomethings Have It Easier
Once the calendar flips to thirty-five, everything shifts. Suddenly, the medical red tape melts away, insurance companies stop asking annoying questions, and surgeons become remarkably accommodating. It is as if society collectively decides that by thirty-five, your brain has miraculously finished baking and you can finally be trusted with your own fallopian tubes.
The Magic of the Thirty-Five Benchmark
There is nothing intrinsically holy about the mid-thirties, except that it represents the twilight of the standard obstetric timeline. Clinicians view thirty-five as the onset of advanced maternal age (what used to be called a geriatric pregnancy), meaning they are far less precious about preserving your fertility against your will. As a result: the conversation shifts from "Are you sure?" to "Let's get this scheduled for next Tuesday." It is a massive double standard, but smart patients use it to their advantage.
When Career and Clarity Converge
By the time you hit thirty-six, your lifestyle has usually hardened into concrete. You know your income trajectory, you know your partner's quirks (or your deep satisfaction with singlehood), and you have watched your friends raise toddlers, which gives you a visceral, unromanticized view of what parenting actually entails. Your decision is no longer theoretical. Honest to God, experts disagree on whether this mental clarity is due to neurological maturity or just sheer exhaustion from surviving a decade in the modern economy, but the outcome is identical.
Comparing Permanent Cuts to Temporary Shields
Before you commit to a permanent surgical alteration of your pelvic anatomy, you have to look at the other options on the shelf. This is where the debate gets incredibly fierce among gynecologists.
The IUD Versus the Scalpel
The modern hormonal intrauterine device, like the Mirena, boasts a failure rate of less than zero point two percent, making it statistically more effective than a traditional tubal ligation, which sits at roughly zero point five percent failure over a year of use. Think about that for a second. A small piece of plastic inserted during a ten-minute office visit protects you better than an invasive surgery requiring general anesthesia and three days of recovery on the couch. Except that an IUD eventually expires, and you have to go back to the clinic to get it ripped out and replaced, which is its own special brand of torture. For a woman of thirty-two who wants an absolute guarantee until menopause, that temporary shield feels like a half-measure.
The Realities of Surgical Risk
Tubal ligation is a laparoscopy, a real surgery requiring a camera through your belly button and gas pumped into your abdomen that leaves you with shoulder pain for forty-eight hours. It carries a small but genuine risk of bowel perforation or infection. When you look at the long-term cost-benefit analysis, choosing the best age to get your tubes tied means weighing whether your body can easily bounce back from anesthesia. A twenty-five-year-old will be jogging again by Friday; a forty-year-old might need the full weekend plus a few extra days of heating pads and quiet. But the peace of mind? That lasts forever.
Common misconceptions surrounding permanent sterilization
The myth of the absolute age threshold
You have likely heard that medical professionals possess a secret, rigid chronological milestone before which they automatically deny requests for tubal ligation. The problem is that no universal, legally mandated minimum age exists across the global healthcare landscape outside of standard adult consent laws. Doctors evaluate systemic readiness rather than arbitrary calendar dates. Some clinics hesitate when confronting a twenty-four-year-old patient, yet they readily approve a thirty-year-old with identical reproductive certainty. This disparity stems from clinical anxiety regarding post-procedure regret. Statistics indicate that nulliparous individuals sterilized under age thirty experience the highest rates of subsequent dissatisfaction, hovering near twenty percent. Conversely, that probability plummets to under six percent for individuals who undergo the procedure after crossing the thirty-five-year milestone. Age acts as a statistical proxy for psychological stability, not an insurmountable legal barrier.
The illusion of easy reversibility
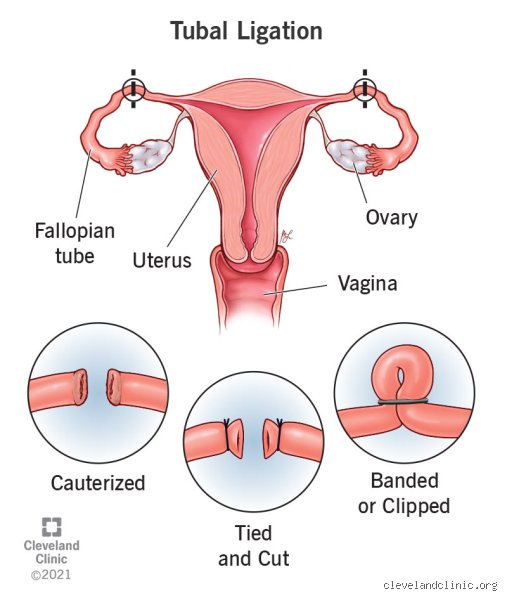
Let's be clear about the mechanics of fallopian micro-surgery. Many patients schedule consultations operating under the assumption that a surgical reversal functions like flicking a simple toggle switch. Except that rejoining severed, cauterized, or clipped anatomical pathways requires intricate microsurgical re-anastomosis. This secondary intervention demands profound financial investment and offers zero guarantees of success. Why gamble with such permanent structural alterations? Success rates for restoring fertility hover unpredictably between thirty and eighty percent, heavily contingent upon the specific destruction method utilized during the initial operation. If you harbor even a microscopic shred of doubt about your future family configuration, choosing what is the best age to get your tubes tied becomes a secondary issue to selecting a highly reliable, reversible long-acting contraceptive instead.
The hidden immunological and hormonal reality
Ovarian reserve dynamics and surgical proximity
Medical literature frequently overlooks how local pelvic vascular networks alter long-term endocrine health post-surgery. When a surgeon applies bipolar coagulation or excises the fallopian structures completely, the localized collateral blood supply feeding the ovaries can occasionally experience transient disruption. This subtle vascular alteration does not trigger immediate menopause. However, it can potentially accelerate micro-fluctuations in localized tissue perfusion. Did you know that some cohort studies tracking patients five years post-sterilization noted minor variations in anti-Mullerian hormone levels among individuals who underwent the procedure in their early twenties? The issue remains that disrupting this delicate web of capillaries might theoretically influence the timing of your natural climacteric transition, albeit by mere months. It highlights why timing this intervention requires analyzing your baseline ovarian vitality, particularly if you possess a familial history of premature ovarian insufficiency.
Frequently Asked Questions
What is the absolute best age to get your tubes tied to minimize long-term psychological regret?
Comprehensive data compiled by the Crest longitudinal study indicates that waiting until at least age thirty-one dramatically optimizes long-term satisfaction outcomes. Patients who finalize this permanent decision between the ages of thirty-five and forty-four report a regret statistic of merely 5.9 percent over fourteen years of post-operative tracking. Conversely, electing for permanent sterilization at age twenty-five or younger propels that specific psychological risk upward to an alarming 20.3 percent. This stark divergence demonstrates that cognitive maturity and stable lifestyle consolidation heavily mitigate subsequent second-guessing. As a result: waiting until your third decade provides the necessary emotional runway to ensure your choice aligns with long-term reality.
Does age significantly impact the statistical failure rate of fallopian tube sterilization?
Youth strangely increases the probability of mechanical failure due to the body's robust, aggressive tissue regeneration capabilities. Young statistics reveal that individuals under the age of twenty-eight experience a ten-year cumulative failure rate of approximately thirty-six per one thousand procedures when using specific bipolar coagulation methods. For individuals over the age of thirty-five, that specific failure rate drops significantly to below twelve per one thousand instances. The body simply becomes less adept at spontaneous anatomical recanalization as the natural aging process advances. Consequently, choosing a later biological window inherently maximizes the absolute contraceptive efficacy of the operation itself.
How does your age at sterilization affect the long-term risk of requiring a subsequent hysterectomy?
Data suggests an unexpected correlation between youthful sterilization and a subsequent elevated probability of undergoing major uterine excision surgery later in life. Women who undergo fallopian ligation before reaching thirty are statistically four times more likely to get a hysterectomy within the subsequent decade compared to those who delay the procedure. This phenomenon does not stem from direct surgical damage to the uterus itself during the ligation. Instead, it occurs because younger individuals are statistically more prone to developing independent benign gynecological issues like heavy bleeding or endometriosis over their remaining reproductive years. It illustrates that early surgical choices often intersect with complex, unpredictable pelvic pathologies as you age.
A definitive perspective on your reproductive timeline
We need to stop treating this deeply personal medical milestone as a purely chronological hurdle. The search for what is the best age to get your tubes tied must prioritize your psychological autonomy over arbitrary societal expectations or rigid clinical hesitation. Yet, ignoring the hard medical data regarding youthful regret rates and tissue regeneration capabilities is equally reckless. My firm stance is that entering your early thirties represents the absolute sweet spot where biological stability, psychological certainty, and low failure rates perfectly converge. But let's acknowledge our collective analytical limits; no statistical model can ever perfectly predict your personal evolution or future relationship dynamics. In short, choose the moment where your current identity feels entirely concrete, absolute, and utterly independent of external pressure.