The All-or-Nothing Reality of Total Microbial Elimination
Microbiology does not tolerate gray areas. When a surface or an instrument is sterile, it means there is an absolute zero probability of microbial survival, a standard formally measured as a Sterility Assurance Level of 10 to the minus 6 power. Honestly, it is unclear why some industry marketing slicks still hint at "partial sterilization" because, frankly, that is a mathematical and biological impossibility. You cannot have a partially dead endospore. The thing is, achieving this absolute blank slate requires destroying the most rugged entities on Earth, such as Geobacillus stearothermophilus, a beast of a bacterium that laughs at standard boiling temperatures.
The Broad Umbrella of Elimination Methods
Sterilization is the macro-concept, the ultimate target. To reach it, scientists and medical professionals deploy an arsenal of different energy types depending entirely on what material they are trying to clean without destroying the substrate itself. Think about it. You cannot throw a delicate polymer catheter or a heat-sensitive pharmaceutical solution into a blistering oven or a pressure cooker. Because of this material vulnerability, the industry has spent the last century perfecting alternative pathways—chemical baths, toxic gases, intense radiation, and mechanical filtration—to hunt down microscopic life where heat would simply melt the equipment. But the issue remains that each alternative brings its own logistical nightmare, toxic footprint, or staggering utility bill.
Enter the Autoclave: High-Pressure Steam Decontamination Explained
Now, where it gets tricky for newcomers is understanding the autoclave itself. This is not just a glorified kitchen pressure cooker, though Charles Chamberland actually invented the modern prototype back in 1879 by adapting exactly that concept. An autoclave is a heavy-duty, pressure-sealed chamber designed to subject instruments to physical forces that tear proteins apart at a molecular level. It operates on a deceptively simple principle: water boils at 100 degrees Celsius under normal atmospheric pressure, which is ambiently 14.7 pounds per square inch at sea level, but if you artificially spike that pressure inside a sealed steel vault, you force the boiling point of the water—and the temperature of the resulting steam—to skyrocket. Saturated steam under pressure becomes a kinetic weapon, transferring latent heat into cell walls far more efficiently than dry air ever could.
The Magic Numbers of the Standard Cycle
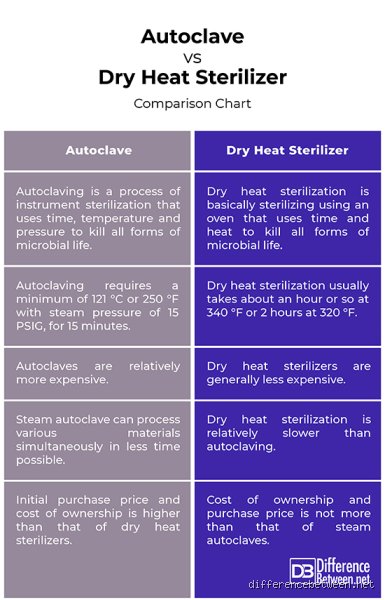
To kill the toughest hitchhikers, a standard gravity-displacement autoclave cycle must hit a baseline of 121 degrees Celsius while maintaining 15 pounds per square inch of gauge pressure for a minimum of 15 to 20 continuous minutes. That changes everything. Why do these specific parameters matter so much? Because dry heat at that same temperature would require hours to achieve the same result, yet moist heat causes rapid, irreversible coagulation and denaturation of structural proteins and enzymes within the pathogen. And that is the secret sauce. For heavier, denser loads like thick biohazard waste bags or large trays of stainless steel surgical tools, technicians must bump the settings up to 134 degrees Celsius at 30 pounds per square inch for a shorter, sharper 3 to 4 minutes. People don't think about this enough, but skipping even 60 seconds of that exposure window can leave millions of viable microbes intact at the center of a dense load.
The Mechanical Workflow Inside the Chamber
How does the machine actually pull this off? First, the ambient air must be aggressively purged from the chamber because air pockets act as insulators, blocking the steam from directly kissing the cold surfaces of your instruments. In modern pre-vacuum autoclaves, a powerful pump sucks the chamber dry of air before pulsing the steam inside. Once the target pressure and temperature are reached, the dwell period begins, during which the machine monitors the environment with surgical precision. Afterward, the steam is vented, the pressure drops back to normal, and a drying cycle kicks in so you do not pull out wet packs, which can inadvertently draw environmental bacteria through paper wrapping via a wicked phenomenon known as wicking.
Comparing Moist Heat to Alternative Sterilization Pathways
While autoclaving reigns supreme as the gold standard for hospital sterilization, we are far from it being a universal cure-all. If you tried to sterilize a sensitive protein-based medication or a delicate optic lens using 121-degree steam, you would end up with a useless puddle of ruined components. This brings us back to the core difference between sterilization and autoclaving: the latter is just one tool in a very diverse shed.
Chemical and Gas Alternatives for Delicates
When heat is out of the question, industries turn to gaseous sterilization, most notably Ethylene Oxide gas, which alters microbial DNA through a process called alkylation. Hospitals use this for heat-sensitive endoscopes, except that Ethylene Oxide is highly carcinogenic and requires a lengthy aeration period—sometimes up to 12 hours—to ensure the toxic gas dissipates safely from the treated gear. Another major player is hydrogen peroxide gas plasma, which utilizes radiofrequency or microwave energy to disrupt cell functions at much lower temperatures, typically below 50 degrees Celsius, making it perfect for complex electronics.
Radiation and Physical Filtration
Then we have the heavy artillery used by industrial manufacturers of single-use plastics, like those disposable syringes or Petri dishes you see in every clinic. They use gamma rays or electron beams, ionizing radiation that shatters microbial genetic structures on contact. But what if you are working with a liquid pharmaceutical fluid that cannot withstand heat or chemicals? You resort to membrane filtration with a pore size of 0.22 micrometers, physically trapping bacteria and fungi while letting the liquid pass through untouched. As a result: you achieve a sterile product without ever altering its chemical makeup.
How Material Composition Dictates the Sterilization Strategy
Choosing between autoclaving and other sterilization methods requires a deep understanding of material science. Stainless steel, polypropylene plastics, and borosilicate glass are the beloved workhorses of the autoclave world because they shrug off the intense thermal stress and moisture. But the real world is messy, and choosing the wrong pathway can have catastrophic consequences for research integrity or patient health.
When Heat Destroys the Objective
Consider the delicate world of tissue culture or vaccine manufacturing. If you expose a growth medium containing vitamins or heat-labile serum to an autoclave cycle, you will caramelize the sugars and denature the essential proteins, rendering the broth completely useless for growing cells. Experts disagree on the exact thresholds for certain complex enzymes, but the consensus remains that physical filtration is the safer bet here. In short, knowing the difference between sterilization and autoclaving protects both your budget and your biological samples from preventable ruin.
Common Mistakes and Misconceptions Regarding Microbial Elimination
The Dangerous Fallacy of Over-reliance on Temperature Alone
You cannot simply crank up the heat and assume everything on your surgical tray is completely sterile. This is where many technicians stumble. Heat represents just a single variable in a multifaceted equation. Let’s be clear: pressure acts as the real heavy lifter during wet sterilization processes. Without adequate pressure, steam fails to reach the critical penetration depth required to denature stubborn bacterial endospores. Achieving true medical-grade sterility requires a precise choreography of parameters. If your autoclave chamber fails to purge trapped air pockets completely, the core temperature drops precipitously within those invisible voids, leaving pathogens perfectly alive. The problem is that many operators look at a digital readout showing 121°C and assume the job is done, ignoring the laws of thermodynamics.
Confusing Cleanliness with Absolute Sterility
An object cannot be semi-sterile. It is a binary condition, yet laboratory newcomers frequently conflate rigorous disinfection with actual sterilization protocols. Washing glassware with high-grade disinfectants removes visible bioburden. Does it kill Geobacillus stearothermophilus spores? Absolutely not. Total eradication of viable microorganisms demands a validated, lethal process. Autoclaving represents a specific, highly reliable method under the broader sterilization umbrella, except that it remains completely useless for moisture-sensitive instruments or hydrophobic powders. Believing that putting a sealed, dry bottle into a steam jacket will sterilize its contents is a recipe for cross-contamination disasters.
Advanced Insights: The Chemistry of Steam Penetration and Expert Calibration
The Latent Heat Secret Weapon
Why do we obsess over saturated steam rather than dry air at identical temperatures? The answer lies in latent heat transfer. When steam contacts a cooler instrument, it condenses instantly. Because of this phase change, it releases massive amounts of thermal energy directly into the cellular walls of the contaminants. Dry heat requires hours to accomplish what pressurized steam manages in mere minutes. Yet, we must acknowledge our limits; this miraculous transfer fails entirely if your steam quality drops below 95% moisture content. Superheated steam behaves exactly like dry gas, rendering your expensive autoclave nothing more than a glorified toaster. Optimizing steam dryness fractions remains the ultimate hallmark of an expert sterilization technician.
Frequently Asked Questions
Can you use autoclaving as the universal standard for all medical waste sterilization?
No, because specific materials like volatile chemical compounds, toxic pharmaceutical waste, and low-density plastics will degrade or release hazardous fumes under high-pressure steam conditions. While autoclaving effectively neutralizes biohazardous tissue and blood samples, it cannot process cytotoxic drugs or radioactive materials which require specialized incineration instead. Statistics show that roughly 20% of biomedical laboratory waste streams contain mixed hazards that are completely incompatible with steam exposure. Proper segregation must occur beforehand so that items requiring alternative sterilization vs autoclaving pathways are routed correctly. For instance, non-porous plastics might melt entirely at the standard 134°C cycle, ruining the entire autoclave chamber and necessitating expensive repairs.
What is the standard holding time and pressure required for a validated autoclave cycle?
The baseline medical standard dictates exposing items to saturated steam at a temperature of 121°C for at least 15 minutes under a gauge pressure of 15 pounds per square inch, which equates to roughly 103 kilopascals. Alternatively, flash sterilization cycles can utilize a elevated temperature of 134°C at 30 pounds per square inch for a much shorter duration of just 3 to 4 minutes. These parameters are calculated specifically to achieve a safety assurance level reducing the microbial population by six logarithmic orders of magnitude. Which begs the question: are you regularly verifying these metrics with calibrated biological indicators? Relying solely on chemical tape changes is an unreliable way to guarantee that saturated steam under pressure actually penetrated the center of large fabric packs.
How do validation protocols differ between general sterilization techniques and specific autoclaving methods?
General sterilization validation encompasses diverse testing matrices for ethylene oxide gas, gamma radiation, or hydrogen peroxide plasma, each focusing on different chemical or physical penetration vectors. Autoclave validation specifically narrows its focus to thermal mapping and mechanical pressure readings using specialized thermocouple arrays placed throughout the physical chamber. Technicians must run routine spore tests utilizing Geobacillus stearothermophilus compliance ampoules, which are specifically resistant to moist heat. In contrast, dry heat sterilization validation relies on Bacillus atrophaeus due to its unique resistance to desiccation. As a result: an facility must maintain distinct validation logs for every unique microbial destruction mechanism utilized across their departments.
A Definitive Stance on Decontamination Paradigms
We must stop treating these two distinct terms as interchangeable jargon because doing so erodes the rigorous standards required in modern clinical and laboratory environments. Sterilization remains the uncompromising objective, while autoclaving is merely one highly effective, time-tested weapon among a larger arsenal of methodologies. Choosing the wrong tool out of sheer convenience risks patient lives and compromises experimental integrity. But the industry continues to cut corners by favoring speed over scientifically validated exposure times. We firmly maintain that a blanket approach to decontamination is inherently dangerous. In short, true professional competence requires a deep, granular understanding of how specific pathogens react to distinct physical forces rather than relying on a generalized hope that heat fixes everything.