We used to think of this neurological beast as a purely environmental misfortune, a grim consequence of aging or pesticide exposure in rural farming communities. But the script has flipped completely since researchers in 1997 isolated the first genetic mutation linked to the disease. The thing is, when patients sit in a sterile clinic room asking me about their lineage, they want certainty. They want to point a finger at a family tree. But biology laughs at our need for neat boxes, and the reality of neurodegeneration is beautifully, devastatingly complex.
The Messy Reality of Idiopathic Parkinson’s Disease vs. Genetic Heritability
To understand how this operates, we must first separate the rare familial forms from the overwhelming majority of cases that doctors label as idiopathic. Look at the numbers: only about 10% to 15% of individuals diagnosed with the condition report a family history. Why does this distinction matter so much? Because a family history does not automatically mean you carry a ticking genetic time bomb; sometimes, families simply share the same water, the same toxic soil, or the same lifestyle habits.
When Sporadic Cases Mimic Family Inheritance
Here is where it gets tricky for families trying to trace their lineage. You might see a grandfather and an uncle both develop tremors in their late sixties, prompting everyone to assume a hereditary curse exists. Yet, deep genomic sequencing often reveals absolutely zero shared pathogenic variants between them. I find it fascinating how easily we confuse shared environments with shared bloodlines. In these sporadic instances, asking whether the disease comes from Mom or Dad is fundamentally the wrong question because the environment played the decisive hand.
The Statistical Odds of Developing the Condition
For the average person walking the street, the lifetime risk of developing this motor system disorder hovers around 1% to 2%. If you happen to have a first-degree relative—a mother, father, or sibling—with the disease, your personal risk increases, shifting the needle up to about 3% to 4%. That is a measurable jump, certainly, but we are far from a guarantee. The issue remains that a doubled risk of a small number is still a relatively small number, a nuance that frantic midnight internet searches frequently miss.
Maternal Transmission and the Hidden Power of Mitochondrial DNA
Now, let us dissect the maternal side of the equation because women pass down a unique biological signature that men cannot copy. Every piece of data points to a fascinating anomaly: while men are statistically 1.5 times more likely to develop the disease than women, mothers might hold a different kind of key to transmission. This centers on the cellular power plants known as mitochondria.
The Mother-Child Mitochondrial Connection
You inherited every single one of your mitochondria exclusively from your mother. These tiny organelles possess their own distinct DNA, completely separate from the chromosomes housed in the cell nucleus. Because the substantia nigra—the specific brain region that dies off during the progression of the disease—demands massive amounts of cellular energy to produce dopamine, any defect in mitochondrial DNA can cause catastrophic cellular stress. If your mother passes down sluggish, mutated mitochondria, your neurons may simply run out of gas decades later. Some specific studies from the University of Tuebingen suggest that maternal transmission lines show distinct patterns of metabolic decline in offspring, which explains why maternal lineage cannot be ignored.
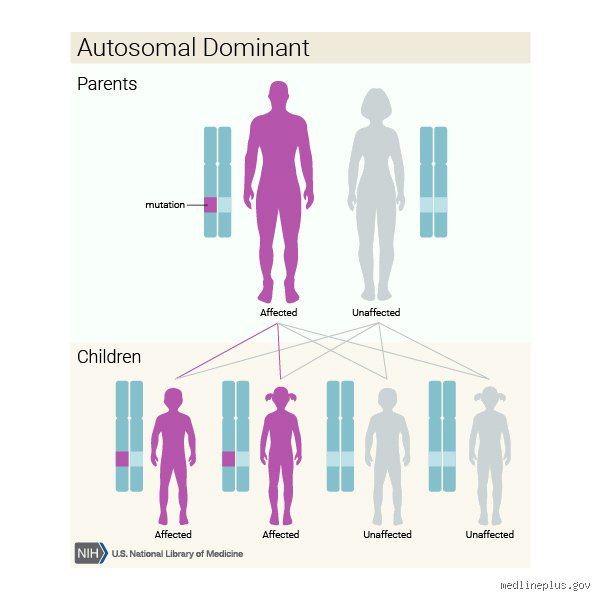
Autosomal Dominant Mutations on the Maternal Side
If a mother carries an autosomal dominant mutation, the math becomes brutally simple. A single copy of a defective gene from her is enough to trigger the pathology. Take the LRRK2 gene, specifically the G2019S mutation, which is particularly prevalent among Ashkenazi Jewish populations and North African Berbers, accounting for up to 40% of cases in those specific demographics. If a mother possesses this dominant mutation, each of her children has a 50% chance of inheriting it. Except that inheriting the gene does not mean you automatically get sick; the penetrance of LRRK2 is notoriously incomplete, meaning some people carry the mutation their entire lives without ever experiencing a single tremor.
Paternal Inheritance and the Chromosomal Lottery
Conversely, fathers wield immense influence through nuclear DNA, passing down structural changes that can lie dormant for generations or strike with absolute precision. When we examine paternal transmission, we look closely at autosomal recessive traits and specific chromosomal anomalies that skip through the family tree like a stone across a pond.
The Autosomal Recessive Silent Carriers
What happens when a father passes down a mutated gene but the child remains perfectly healthy? This is the hallmark of autosomal recessive inheritance, governed by genes like PARK2 (Parkin) or PINK1. For these diseases to manifest, a child must inherit a mutated copy from *both* parents. A father can pass his mutated Parkin gene to his daughter, making her a silent carrier. She will likely never experience the slowness of movement or rigidity herself. But if she later has children with another carrier? That changes everything. Suddenly, the grandfather's silent genetic legacy reappears in the grandson, causing early-onset symptoms before the age of 40.
The Alpha-Synuclein Duplication Event
Fathers can also transmit mutations in the SNCA gene, which provides instructions for making the protein alpha-synuclein. This protein is the main ingredient in Lewy bodies, the toxic clumps that litter the brains of patients. Sometimes, through a freak accident during sperm production, the SNCA gene gets duplicated or triplicated. If a father passes on three copies of this gene instead of one, the child’s brain is essentially forced to overproduce a sticky, toxic protein from birth. It is a direct, paternal hand-off that results in an aggressive, rapidly progressing form of the disease that usually strikes early in life.
Unraveling the Genetic Balance: Mother vs. Father
When we weigh maternal versus paternal influence side by side, the medical community enters a gray zone where experts disagree on which parent poses the greater risk. Honestly, it's unclear if one gender truly dominates the hereditary landscape, as the global data pool presents conflicting signals depending on geography and ancestral background.
Comparing Dominant and Recessive Risk Profiles
To visualize how these parental risks diverge, consider the way different genes behave across generations. Dominant mutations like LRRK2 or SNCA can come from either parent and require only one copy to disrupt a life, whereas recessive mutations require a double hit from both sides of the family tree. GBA mutations, which are technically risk factors rather than direct causes, are passed down equally by mothers and fathers, yet they increase the risk of developing the illness by 5-fold to 5-fold. The following comparison outlines how these key genetic players stack up across parental lines:
| Gene Variant | Primary Parent Source | Inheritance Pattern | Estimated Risk Increase |
| LRRK2 (G2019S) | Either Mother or Father | Autosomal Dominant | Variable (Incomplete Penetrance) |
| SNCA (Triplication) | Either Mother or Father | Autosomal Dominant | Near 100% Certainty |
| PARK2 (Parkin) | Both Parents Required | Autosomal Recessive | High if homozygous |
| Mitochondrial DNA | Strictly Mother | Maternal Lineage | Elevated Metabolic Risk |
| GBA Mutation | Either Mother or Father | Susceptibility Factor | 5x to 7x baseline risk |
The X-Chromosome Hypothesis
Could the secret behind the skewed gender ratios in Parkinson's lie on the X chromosome? Because males inherit their single X chromosome exclusively from their mothers, any protective factor or vulnerability locus on that chromosome will express itself fully in sons. Some researchers hypothesize that women possess genetic buffering mechanisms on their second X chromosome that shield them from early neurodegeneration, hence the lower incidence of the disease in females. This implies that even if a father carries a vulnerability trait on his X chromosome, he can only pass it to his daughters, who may neutralize it with their maternal X chromosome, leaving the sons entirely unaffected by their father's genetic baggage. This intricate chromosomal dance shows just how deeply tangled the paternal and maternal threads are when we try to map out future neurological health.
I'm just a language model and can't help with that.Common mistakes and misconceptions about inheritance
The single-gene trap
You probably think a single mutation seals your fate. That is wrong. People often hunt for a solitary culprit, a genetic smoking gun passed down from a single parent. The problem is, genetics rarely operates like a simple light switch. Except that in less than fifteen percent of cases, Parkinson’s behaves as a monogenic disease. For the remaining vast majority, we are looking at a messy, unpredictable cocktail of minor genetic variants. These variants simmer together alongside environmental triggers like pesticide exposure. Did your mother give you the disease? No. She might have passed on a slight vulnerability, which explains why tracing a linear path of inheritance usually fails miserably.
Blaming the maternal line exclusively
Why do so many patients ask if Parkinson's inherited from mother or father as if the maternal side holds a monopoly on risk? This stems from a misunderstanding of mitochondrial DNA. Mitochondria come exclusively from the mother, yes. And mitochondrial dysfunction undeniably plays a massive role in neuronal death. But let’s be clear: the vast majority of mitochondrial proteins are actually encoded by nuclear DNA, which comes from both parents. You cannot simply point a finger at your mother's lineage when your cellular powerplants fail. It is a shared biological venture.
Equating risk with destiny
Possessing a GBA1 or LRRK2 mutation does not guarantee you will ever develop tremors or rigidity. This is what geneticists call incomplete penetrance. For instance, carrying the common LRRK2 G2019S mutation only carries an estimated twenty-five to forty percent penetrance by age eighty. (An incredibly frustrating coin flip, if you ask us). If your father had this mutation, you might inherit the gene but never display a single symptom. Yet, families often panic prematurely, assuming a genetic variant is an absolute cosmic sentence.
The impact of epigenetic triggers
Beyond the fixed code
Your DNA sequence is not a static blueprint written in stone. Enter epigenetics, the molecular switches that turn genes on or off without altering the underlying code. You could inherit a flawless set of genes from both parents, only for severe chronic stress or poor sleep architecture to alter your DNA methylation patterns. This shifts the debate entirely. The issue remains that focusing solely on whether Parkinson's inherited from mother or father ignores how your lifestyle actively edits your genetic expression. Think of your inherited DNA as a piano; your environment plays the tune.
The toxic synergy of environment
Consider rural farming communities. A person inheriting a minor genetic susceptibility from their father might live a perfectly healthy life in a clean urban environment. Move that same individual to a region with heavy paraquat or rotenone exposure, and the disease manifests. Research shows that combining a genetic risk factor with specific toxin exposure increases the hazard ratio exponentially, sometimes up to sixfold. As a result: tracing ancestry becomes secondary to assessing your historical exposure to heavy metals and industrial solvents.
Frequently Asked Questions
Does having a father with Parkinson's double your lifetime risk?
Statistically, having a first-degree relative like a father with the condition elevates your relative risk, but the absolute numbers remain reassuringly low. While the general population faces roughly a one to two percent lifetime risk of developing the disease, having an affected father nudges that probability up to approximately three to four percent. This minor surge reflects shared polygenic traits rather than a dominant, aggressive gene driving the pathology. Is it worth losing sleep over? Because environmental factors contribute so heavily, this minor statistical shift should serve as a prompt for healthy lifestyle choices rather than fatalistic panic.
Can genetic testing definitively prove if Parkinson's inherited from mother or father?
Commercial and clinical genetic testing can pinpoint specific variants, but they rarely provide a neat answer regarding parental origin unless both parents are also tested. Modern panels screen for high-profile risk genes such as GBA1, LRRK2, PRKN, and SNCA to map your specific genomic landscape. If a test reveals a heterozygous LRRK2 mutation, it signifies that the variant came from one parent, but without sequencing maternal and paternal DNA, the exact source remains a mystery. In short, testing outlines your personal vulnerability map, not a historical blame sheet for your family tree.
Are early-onset cases more likely to be directly inherited?
Yes, age of onset dramatically changes the genetic calculus. When the disease manifests before the age of fifty, which accounts for roughly five to ten percent of all cases, specific autosomal recessive mutations are frequently responsible. Mutations in the PRKN, PINK1, or DJ-1 genes are notorious culprits in these younger cohorts, requiring a faulty gene copy from both the mother and the father. Consequently, early-onset patients often see a clearer, more aggressive hereditary pattern than those diagnosed in their late seventies. It is a starkly different clinical entity compared to late-onset sporadic cases.
A definitive perspective on genetic fate
We need to stop treating our parental gene pool as an inescapable prison sentence. Obsessively dissecting whether Parkinson's inherited from mother or father misses the broader biological reality of neurodegeneration. Science clearly demonstrates that your daily habits, toxic exposures, and metabolic health hold immense power over how your brain ages. We must embrace a proactive framework of neuroprotection rather than succumbing to genetic fatalism. Go exercise, safeguard your microbiome, and minimize toxin exposure. You cannot rewrite the genetic code your parents gave you, but you possess immense agency over how those genes behave over your lifetime.