The Reality Behind the Slang: What Schizophrenia Actually Is
Language matters, yet we ruin it with casual shorthand. When people search online using the truncated term, they are usually looking for answers about schizophrenia, a complex neurodevelopmental disorder affecting roughly 24 million people worldwide according to World Health Organization metrics. The thing is, it is not a split personality. That changes everything when you realize that the clinical reality is far removed from the Dr. Jekyll and Mr. Hyde myth popular culture aggressively peddles. It is a fragmentation of thought processes.
A History of Misunderstanding from Kraepelin to Bleuler
We have been trying to categorize this mental landscape since 1899 when German psychiatrist Emil Kraepelin coined the term dementia praecox to describe a premature dementia. Except that he got it wrong. Later, in 1911, Swiss alienist Eugen Bleuler introduced the term schizophrenia—derived from the Greek words for splitting and mind—to describe the loosening of associations within the brain. Yet the issue remains that the public still confuses this loosening with having multiple identities, which is actually Dissociative Identity Disorder. Honestly, it's unclear why this misconception persists so stubbornly when medical literature has been shouting the truth for over a century.
The Statistical Scope of a Global Condition
Data paints a stark picture. The onset typically hits young adults between the ages of 16 and 30, with men often showing symptoms earlier than women. In places like London or New York, urban clinical settings report a slightly higher incidence rate than rural areas, a phenomenon researchers call the urbanicity effect. Why does concrete pavement correlate with psychosis? Experts disagree on the exact mechanism, but the stress of high-density living combined with genetic vulnerabilities seems to trigger the latent condition. You cannot ignore the numbers: it affects approximately 1 in 300 people globally, making it less common than depression but vastly more disruptive if left unmanaged.
The Prodromal Phase: Catching the Shadows Before the Storm
You don't just wake up one morning completely detached from reality. There is a preamble, a slow-burning fuse that psychiatrists call the prodromal phase. This is where it gets tricky because the initial indicators look exactly like standard teenage angst or a severe bout of burnout. You start pulling away from friends. Your grades at university drop from straight A’s to failing marks. But people don't think about this enough: isolation isn't just about wanting alone time; it is an inability to process social cues that suddenly feel overwhelming, like trying to read a map while riding a roller coaster.
Subtle Cognitive Declines and the Loss of Working Memory
Long before the loud symptoms arrive, the brain’s executive functioning begins to fray. You might notice that you can no longer follow the plot of a simple movie or remember what you read three sentences ago. This is a deficit in working memory, a core feature that standard antipsychotic medications historically fail to fix. I argue that these cognitive symptoms are actually more debilitating than the hallucinations themselves because they strip away a person's ability to maintain employment or navigate a grocery store. But try explaining to a doctor that your brain feels like it’s running on a dial-up internet connection while everyone else is on fiber optic.
The Uncanny Valley of Perceptual Distortions
Then comes the altered sense of self. Colors might seem unnaturally vivid, or the hum of the refrigerator in your apartment might suddenly sound like a coded message meant solely for you. It is an experience of heightened salience, where the brain attaches profound significance to completely random external stimuli. You are walking down a street in Chicago and notice a red car parked at the curb—suddenly you are convinced it is a surveillance vehicle. It is not a full-blown delusion yet, but rather a creeping feeling that the backdrop of life has become sinister.
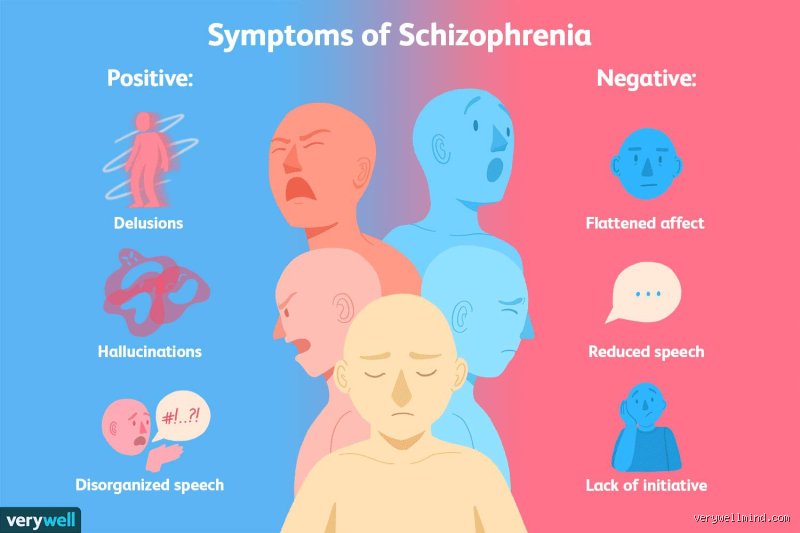
The Positive Symptoms: When the Brain Manifests Too Much
When asking how do you know if you have schitzo, clinicians look heavily at positive symptoms, which are behaviors or experiences added to a person’s psychological baseline. These are the headline-makers. They are loud, terrifying, and completely real to the person experiencing them. Because the brain's internal monitoring system misfires, thoughts are perceived as external auditory inputs.
Auditory Hallucinations and the Internal Cacophony
Hearing voices is the classic hallmark. These are not merely intrusive thoughts or the standard internal monologue we all possess. They are distinct, externalized sounds that seem to originate from the next room or from the ceiling vents. Sometimes it is a single voice commenting on your actions in real-time, pointing out how poorly you are washing the dishes; other times it is a hostile chorus demanding obedience. Imagine living with a permanent, malicious radio broadcast playing inside your skull that you cannot turn off—how long could you maintain your sanity under that kind of relentless acoustic bombardment?
Delusional Premises and the Trap of Immutable Logic
Delusions are fixed, false beliefs that remain completely unshakable even when confronted with undeniable contrary evidence. They frequently take a persecutory turn. You might become convinced that the food your mother cooks is laced with heavy metals, or that a microchip was implanted in your molar during a routine dental visit in 2024. The terrifying thing about delusions is their internal consistency. If you accept the initial premise—that the government is actively tracking your thoughts—then hiding your head in aluminum foil or destroying your smartphone becomes a completely logical, self-protective action, which explains why trying to argue someone out of a delusion never works.
Disorganized Thought and the Phenomenon of Word Salad
The structural integrity of language collapses when psychosis takes hold. This manifests as formal thought disorder. A conversation with someone entering acute psychosis can feel like trying to decipher a broken code because their ideas jump from one topic to an entirely unrelated one without any logical bridge. In severe cases, this degrades into word salad, a jumble of neologisms and random nouns that defies syntax. As a result: communication breaks down entirely, leaving the individual profoundly isolated within their own impenetrable linguistic fortress.
The Negative Symptoms: The Quiet Erasure of the Self
If positive symptoms are an explosion of excess mental activity, negative symptoms are the hollowed-out crater left behind. They represent the removal of normal human functions. Families often find these more heartbreaking to witness because the person they knew seems to slowly evaporate into a shadow of themselves, leaving behind an empty shell that rarely speaks or moves.
Avolition and the Complete Paralysis of Willpower
This is not laziness. Avolition is a total, neurological destruction of desire and motivation. A person might sit in a chair for twelve hours straight, staring at a blank wall, completely unbothered by the passage of time or the grime accumulating around them. They want to get up—or rather, they know they should get up to shower or eat—but the neurological pathway that translates an intention into physical movement is entirely severed. We are far from a simple lack of discipline here; this is a profound deficit in the brain's dopamine-driven reward system.
Affective Flattening and Alogia
The emotional palette turns entirely gray. When you speak to someone experiencing affective flattening, their face remains completely immobile, like a plaster mask, and their voice drops to a monotonous drone devoid of inflection. They might recount a terrifying hallucination or a joyful memory with the exact same deadpan delivery. Accompanying this is alogia, a poverty of speech where responses are reduced to brief, one-word answers. You ask how their day was, and after a long, agonizing pause, they mutter a single syllable. In short: the expressive capacity of the human spirit is dialed down to near zero.
Common mistakes and dangerous misconceptions
The split personality myth
Let's be clear: schizophrenia is not dissociative identity disorder. Pop culture has spent decades butcher-shop-editing clinical reality for cheap box office thrills, which explains why the average person still conflates the two. When someone asks how do you know if you have Schitzo, they often incorrectly envision Jekyll and Hyde. The problem is that the actual pathology involves a fracturing of reality, not a multiplication of personas. It is a disintegration of cognitive harmony.
The assumption of perpetual violence
Media tropes love a predictable villain. Yet, statistically, individuals grappling with schizophrenia are exponentially more likely to become victims of violent crime rather than its perpetrators. A shocking fourteenfold increase in victimization risk exists for this population compared to healthy controls. But fear sells newspapers. Society prefers a convenient scapegoat over complex neurological empathy, a reality that complicates genuine diagnosis because terrified individuals stay deeply hidden in their suffering.
Assuming it is a intellectual death sentence
Genius and psychosis frequently tango on the same tightrope. John Nash won a Nobel Prize while navigating profound auditory hallucinations. Diagnosis does not instantly vaporize a person's intellectual capacity or creative spark, except that the medical system sometimes treats patients as static charts rather than dynamic minds. It is a spectrum of neurological diversity, not a uniform descent into cognitive oblivion.
The prodromal phase: An expert vantage point
Catching the whispers before the scream
Psychiatrists look for the prodrome. This is the subterranean, pre-psychotic twilight zone where the disease germinates, often lasting between one to two years before a full-blown break occurs. You might notice a creeping social withdrawal, bizarrely idiosyncratic preoccupations, or a subtle flattening of emotional expression. (Family members usually spot these micro-shifts first, noting that their loved one seems to have drifted behind a pane of smoked glass.) Is it merely an angsty adolescent phase, or are the gears of reality genuinely slipping? Early intervention during this fragile window can radically alter the long-term prognosis, reducing the duration of untreated psychosis which directly correlates with better brain tissue preservation over time.
Frequently Asked Questions
At what specific age do the first symptoms typically manifest?
The timeline is stubbornly gendered and brutally precise. For biological males, the inaugural psychotic break usually strikes between the ages of eighteen and twenty-five, hitting right during the peak of emerging adulthood. Biological females enjoy a slight delay, typically encountering onset between twenty-five and thirty-five, with a secondary post-menopausal spike. Over seventy-five percent of cases become apparent within these specific age brackets, making late-adolescent behavioral shifts highly critical to monitor. As a result: sudden academic collapse or radical personality transformations during college years demand immediate professional psychiatric evaluation rather than mere parental lecturing.
Can lifestyle choices or intense stress trigger the condition?
Stress does not manufacture the illness out of thin air, but it absolutely acts as a high-velocity accelerant. The underlying genetic vulnerability requires an environmental spark, a mechanism beautifully illustrated by the diathesis-stress model. Substance abuse, particularly high-potency cannabis use during brain development, increases the risk of developing the disorder by up to four hundred percent in genetically predisposed teenagers. The issue remains a complex dance of nature and nurture, meaning a chaotic environment can unlock a genetic Pandora's box that might have otherwise stayed permanently sealed.
How do you know if you have Schitzo versus severe clinical depression?
The diagnostic boundary often blurs within a clinical presentation called schizoaffective disorder. Severe depression can feature psychotic elements, such as hearing voices telling you that you are worthless, but these hallucinations remain strictly mood-congruent. True schizophrenia operates independently of your emotional state, delivering bizarre, unprovoked delusions that persist even when your mood stabilizes. Because human suffering resists neat medical boxes, distinguishing between them requires a longitudinal six-month diagnostic tracking period by a certified psychiatrist.
A definitive stance on the diagnostic frontier
We must stop treating schizophrenia as a ghostly, supernatural curse and view it strictly through the lens of aggressive neurobiology. The current diagnostic manual relies far too heavily on subjective behavioral checklists when we should be sprinting toward advanced biomarkers and neuroimaging. Labeling someone based solely on behavioral outputs is an antiquated approach, especially when early therapeutic stabilization can rescue millions of cortical neurons from chronic inflammatory degradation. Waiting for a catastrophic, public psychotic break to occur before initiating aggressive treatment is a systemic medical failure. We need to democratize access to specialized early-psychosis clinics immediately. The human brain is far too complex for us to tolerate medieval stigmas in a modern medical world.