The Grimy Anatomy of a Global Gastrointestinal Crisis
To understand the spread, we have to look past the simple stomach ache. Dysentery is not just diarrhea; it is an inflammatory disorder of the intestine, specifically the colon, resulting in severe diarrhea with blood and mucus in the stool. The thing is, people do not think about this enough as a dual threat. You have bacillary dysentery, caused by Shigella bacteria, and then there is amoebic dysentery, triggered by the protozoan parasite Entamoeba histolytica. They are two entirely different beasts biologically, yet they thrive in the exact same environments.
The Shigella Surge and Amoebic Ambush
Bacteria move fast. Shigella requires an incredibly low infectious dose—sometimes fewer than one hundred organisms are enough to wreck a human digestive tract—which explains why it tears through crowded urban settlements like wildfire. Amoebiasis, by contrast, plays a longer game, often lurking in the colon for weeks before eroding the mucosal lining. But where it gets tricky is the diagnosis. In resource-limited clinics across Bihar or Kinshasa, clinicians lack the diagnostic tools to differentiate between them on the fly. They treat blindly. And that changes everything because treating an amoebic infection with the wrong antibacterial agent achieves absolutely nothing while fueling the terrifying rise of antimicrobial resistance.
The Data Black Hole: Mapping the True Epicenters of Infection
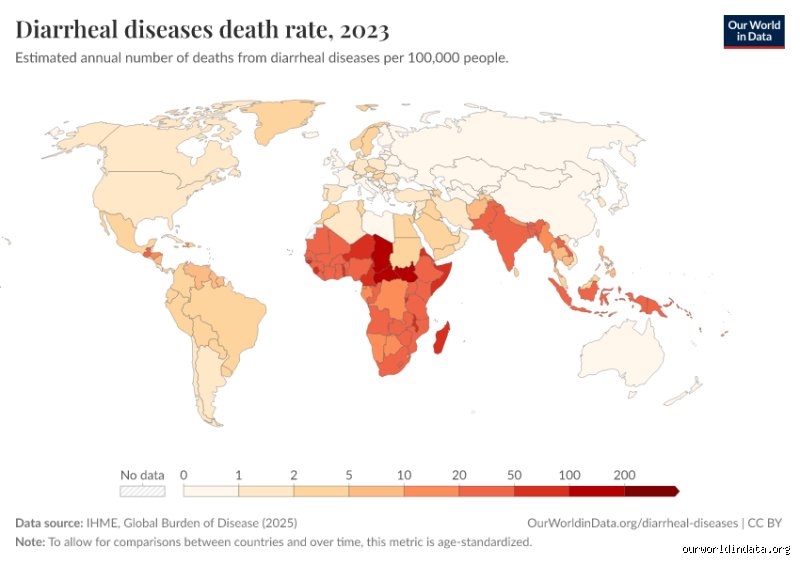
If you cornered an epidemiologist and demanded a straight answer on which country holds the absolute title for the highest case count, they would probably sigh, point toward the Indian subcontinent, and then immediately qualify it with a dozen caveats. India, by virtue of its massive 1.4 billion population and localized sanitation deficits, records millions of acute diarrheal disease episodes annually. Yet, the Global Burden of Disease study often highlights that the highest incidence rates—meaning cases per 100,000 people—frequently suffocate sub-Saharan Africa. The issue remains that national surveillance systems in these regions are fundamentally broken.
The Indian Subcontinent and the Weight of Numbers
Let us look at the raw geography. In 2022, integrated disease surveillance programs in states like West Bengal and Maharashtra logged hundreds of thousands of bloody diarrhea cases, but these are mere fragments of the whole picture. Why? Because the vast majority of rural cases never reach a formal hospital desk. A mother in a remote village near Patna treats her child with local remedies or buys an over-the-counter antibiotic from an unregulated pharmacy booth, meaning that specific case vanishes from official international ledgers. Honestly, it's unclear how many millions are missed every single year, but the sheer volume of transmission in crowded peri-urban slums remains staggering. It is an overwhelming numbers game.
Sub-Saharan Realities and Environmental Triggers
Now, shift the lens to the Democratic Republic of the Congo or Nigeria. Here, the landscape changes from dense urban overcrowding to protracted humanitarian crises where displaced populations drink directly from unprotected rivers. In these environments, Shigella dysenteriae type 1—the notorious epidemic strain that produces the deadly Shiga toxin—finds its perfect playground. Did you know that a single flooded camp can trigger twenty thousand cases in a month? The infrastructure simply cannot cope, creating a vicious loop where the environment itself becomes a biological hazard.
The Molecular Architecture of Transmission
The transmission pathway of these pathogens is remarkably primitive, yet evolutionarily brilliant. It is the classic fecal-oral route, a clinical euphemism for a reality that is deeply unpleasant to contemplate. When infected human waste contaminates local groundwater tables, the pathogen waits silently. A person drinks the water, or eats vegetables washed in it, and the cycle resets. But the biological mechanics inside the host are brutal.
How Shigella Invades the Mucosal Lining
Once the bacteria bypass the stomach acid barrier, they target the epithelial cells of the large intestine. They do not just sit on the surface; they actively hijack the host cell's own cytoskeleton, using cellular actin to propel themselves from one cell to the next like microscopic rockets. This process completely destroys the intestinal wall. The resulting tissue death causes the signature symptom of the disease: micro-abscesses that rupture and spill blood into the intestinal lumen. It is a violent, localized war within the body.
The Amoebic Destructive Cycle
Entamoeba histolytica operates with a different toolkit entirely. It secretes specialized enzymes called cysteine proteinases that literally dissolve human tissue on contact. As a result: the parasite bores deep into the mucosa, creating classic flask-shaped ulcers that can, in severe scenarios, perforate the bowel entirely. This is why amoebic colitis is so feared in tropical medicine circles; if those parasites breach the bloodstream, they travel straight to the liver, causing massive, pus-filled amoebic liver abscesses that require immediate surgical intervention.
Regional Disparities: South Asia Versus Central Africa
Comparing these two macro-regions reveals a fascinating paradox in global health dynamics. South Asia faces a crisis born of density and rapid, unplanned urbanization, where mega-cities outgrow their plumbing faster than municipal governments can lay concrete pipes. Central Africa, however, battles a crisis driven by structural poverty and conflict, where water treatment infrastructure is not just inadequate—it is often non-existent. We are far from achieving global equity in clean water access, and the gut bacteria of the world's poorest populations reflect this failure with perfect, tragic accuracy.
The Urban Slum Paradox
In places like Dhaka or Mumbai, you have high-tech economic hubs sitting mere meters away from open drainage canals. The proximity is jarring. A tech worker and a slum dweller might breathe the same air, but their water worlds are light-years apart. When the monsoon rains hit, these distinctions blur as contaminated water backs up into shallow wells, exposing thousands to Shigella flexneri strains that have slowly adapted to resist common frontline drugs like ciprofloxacin and ampicillin. The bacteria are winning the arms race.
Conflict Zones as Pathogen Incubators
In contrast, the situation in eastern DRC or parts of South Sudan is dictated by displacement. When thousands of people are forced to flee violence and gather in temporary settlements without basic latrines, the sanitation profile collapses instantly. Here, the lack of chlorinated water is not an inconvenience; it is a death sentence, particularly for children under five whose immune systems are already compromised by chronic malnutrition. The pathogens do not care about borders or politics—they just look for the fastest path to a new host.
Common mistakes and misconceptions about shigellosis tracking
The mirage of the perfect database
You probably think looking up which country has the most cases of dysentery is a simple matter of checking a World Health Organization spreadsheet. It is not. Let's be clear: public health data is only as good as the laboratory infrastructure backing it up. Because bloody diarrhea requires a stool culture for definitive identification, nations with robust surveillance networks appear to have massive outbreaks. Meanwhile, a country lacking basic clinics might report nothing at all. The issue remains that we confuse administrative silence with a lack of disease.
Amoebic versus bacillary confusion
Many conflate all bloody stools into a single category. Except that Entamoeba histolytica and Shigella bacteria are entirely different beasts. While amoebic strains cause prolonged misery in tropical zones, Shigella sonnei dominates wealthier, temperate nations. Did you know that the latter spreads like wildfire in daycare centers across Europe and North America? Treating a bacterial infection with antiparasitic drugs because of a bad self-diagnosis is a classic, dangerous blunder.
The stealthy mechanism of asymptomatic transmission
The hidden reservoir in plain sight
Public health officials fixate on patients writhing in agony. Yet, the real driver of hyper-endemic status in regions like Sub-Saharan Africa is the asymptomatic carrier. A person can shed millions of Shigella organisms into their environment without feeling a single cramp, which explains why containment efforts fail so spectacularly. If you only treat the visibly sick, you miss the invisible majority. Our reliance on symptomatic tracking is a massive blind spot that guarantees the pathogen keeps circulating. (And yes, this means your perfectly healthy-looking travel companion could be a walking biohazard).
Frequently Asked Questions
Which country has the most cases of dysentery globally?
Determining an absolute chart-topper is nearly impossible due to underreporting, but India consistently registers massive numbers of bacillary gastrointestinal infections annually. Global health estimates indicate that the broader South Asia region suffers from over 50 million cases of acute bloody diarrhea each year. Poor urban sanitation in mega-cities accelerates the spread of drug-resistant Shigella strains rapidly. Consequently, the raw volume of infections in dense populations puts South Asian nations at the top of epidemiological estimates. As a result: the absolute burden remains heavily concentrated in developing Asian and African nations.
How does antibiotic resistance affect worldwide dysentery tracking?
Superbugs are completely rewriting the global map of diarrheal diseases. In many parts of Southeast Asia, standard frontline treatments like ciprofloxacin have lost over 80 percent of their efficacy against local strains. This creates a terrifying feedback loop where patients remain infectious for longer periods, multiplying the opportunities for transmission. Why are we still treating these lethal pathogens with outdated protocols? When a country loses control of antibiotic efficacy, its infection rates spike dramatically, distorting historic historical data and rendering standard containment strategies completely useless.
Can you contract severe bloody diarrhea in developed countries?
Absolutely, because the pathogen does not care about national borders or GDP. In the United States alone, the Centers for Disease Control and Prevention estimates around 450,000 cases of shigellosis occur every single year. These outbreaks frequently target marginalized communities, crowded institutions, and schools. But the clinical presentation in wealthy nations is often milder due to better baseline nutrition. In short, while it rarely causes the high mortality rates seen elsewhere, the infection is still a major public health nuisance across the West.
A definitive verdict on global gastrointestinal crises
Fixating on a single nation to blame for global contamination misses the point entirely. The reality of deciding which country has the most cases of dysentery is that it reveals more about our broken tracking systems than actual pathology. We must stop pretending that this is a localized tragedy confined to remote tropical villages. Wealthy nations fund shiny laboratories while ignoring the sewage infrastructure collapse in neighboring territories. True eradication demands aggressive infrastructure funding rather than endless passive data gathering. We have the tools to eliminate this ancient scourge, yet we lack the collective political will to deploy them effectively.