Beyond the Anatomy Lab: What We Actually Mean by Pancreatic Insult
The pancreas sits quietly behind your stomach, an oblong organ roughly six inches long that behaves like a dual-functioning factory. It churns out insulin to manage your blood sugar while simultaneously flooding your small intestine with highly corrosive digestive enzymes. Usually, these enzymes remain inert until they exit the organ. But where it gets tricky is when something triggers these juices to activate prematurely while still inside the delicate pancreatic tissue. The organ literally begins to digest itself. It sounds horrific, and honestly, the clinical reality is just as brutal for the 275,000 Americans hospitalized annually with acute episodes.
The Acute Versus Chronic Divide
We need to talk about timing. Acute pancreatitis hits like a lightning bolt, often sending a patient to the emergency room at 3:00 AM with agonizing, radiating back pain that leaves them curled in a fetal position. Most people recover fully within a week. Yet, for a subset of patients, the damage lingers, morphing into chronic pancreatitis, a slow-burning fire that permanently destroys the organ over decades. The issue remains that the transition from a single flare-up to permanent scarring is notoriously unpredictable. Some patients survive three severe acute attacks with zero long-term damage, whereas others develop irreversible chronic disease after a single mild event—experts disagree vehemently on why this threshold varies so wildly.
The Sneaky Role of Asymptomatic Gallstones
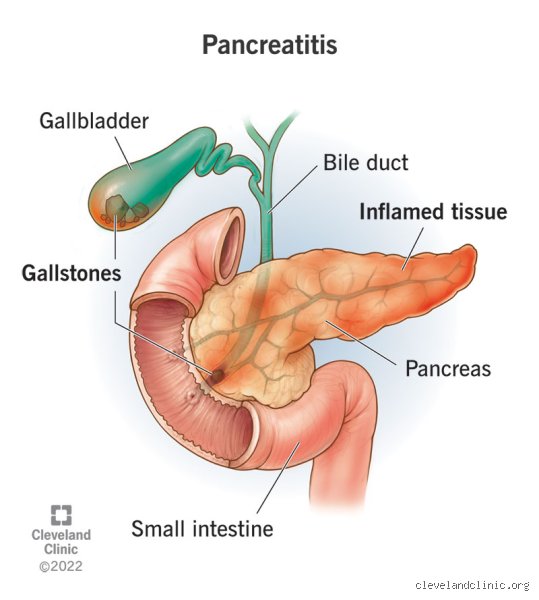
Imagine a tiny, calcified pebble rolling down a narrow pipe. Gallstones, formed from hardened cholesterol in the gallbladder, frequently migrate and get wedged in the common bile duct, effectively blocking the exit ramp for pancreatic enzymes. This mechanical backup triggers roughly 40% of all acute pancreatitis cases globally. The thing is, millions of people walk around with gallstones right now without feeling a single twinge, completely oblivious to the fact that they are sitting on a biological time bomb. If that stone migrates, that changes everything in a matter of minutes.
The Risk Matrix: Unmasking the Most Vulnerable Populations
Who actually ends up in the gastrointestinal ward? The demographics are shifting in ways that catch many clinicians off guard. While older textbooks painted a rigid caricature of the pancreatitis patient, modern epidemiological data from institutions like the Mayo Clinic paints a far more nuanced picture that bridges the gap between DNA and daily habits.
The Metabolic Trap: Alcohol and Triglycerides
Alcohol abuse is traditionally crowned as the primary culprit behind pancreatic inflammation, and it indeed accounts for nearly 30% of acute cases in the United States. But people don't think about this enough: it takes years of heavy drinking—typically more than four or five drinks daily for at least five years—to prime the pancreas for a major blowup. Why? Because alcohol alters the permeability of the pancreatic ductules and increases the protein content of the secretions, creating thick plugs that block flow. And if you couple heavy drinking with high serum triglycerides? You are pouring gasoline on a fire. When fasting triglyceride levels breach the 1000 mg/dL threshold, the blood becomes sludge-like, releasing toxic free fatty acids that shear through pancreatic capillaries, a phenomenon frequently documented in metabolic research clinics from Boston to Berlin.
The Genetic Blueprint: The CFTR and PRSS1 Factors
Some people are dealt a terrible hand at birth. If you inherit a mutation in the PRSS1 gene, your body manufactures a rogue version of trypsinogen that activates far too easily and resists being turned off. This hereditary pancreatitis boasts an astonishing 80% lifetime risk of symptom manifestation, frequently starting in childhood. But we're far from a simple one-to-one genetic deterministic model here. Mutations in the CFTR gene, which is famously responsible for cystic fibrosis, can also cause isolated pancreatic insufficiency and chronic inflammation without ever touching the lungs, an architectural quirk that often leaves adult patients bouncing between misdiagnoses for years before a savvy gastroenterologist orders a comprehensive genetic panel.
Age, Gender, and the Surprising Disparities
Data shows that men are significantly more likely to suffer from alcohol-induced episodes. Conversely, women dominate the gallstone-induced category, particularly during their childbearing years or when undergoing hormone replacement therapy because elevated estrogen naturally increases cholesterol saturation in bile. Is it fair to say middle-aged individuals are the sole targets? Not anymore. Pediatric cases are rising due to the uptick in childhood obesity and subsequent gallstone formation, proving that the traditional age barriers are crumbling rapidly under the weight of modern dietary habits.
The Unsuspected Triggers: Medications and Autoimmune Anomalies
Sometimes the culprit is sitting right in your medicine cabinet. Drug-induced pancreatitis is relatively rare, making up maybe 2% to 5% of cases, but it represents a terrifying diagnostic blind spot for physicians who automatically assume every patient with abdominal pain is a hidden alcoholic.
Pharmaceutical Sabotage
Certain common medications can accidentally trigger an immune response or cause direct cellular toxicity within the pancreas. Azathioprine, an immunosuppressant widely prescribed for Crohn's disease, and certain diuretics like furosemide are well-documented triggers. Even common antibiotics like tetracycline can occasionally provoke a sudden attack. I once reviewed a clinical profile of a 34-year-old marathon runner in Denver who developed severe necrotizing pancreatitis just two weeks after starting a routine course of thiazide diuretics for mild hypertension—a stark reminder that biological vulnerability can hide behind peak physical fitness.
When the Body Attacks Itself
Then we have autoimmune pancreatitis, a bizarre manifestation where the body's immune system decides the pancreas is an invading pathogen. This specific variant is often linked to elevated serum levels of IgG4-positive plasma cells. It mimics pancreatic cancer so perfectly on CT scans that patients are frequently wheeled into major surgeries to remove suspected tumors, only for pathology to reveal a mass of purely inflammatory cells that could have been completely melted away with a simple, inexpensive course of oral steroids.
Weighing the Odds: The Interplay of Smoking and Obesity
We often treat risk factors as isolated columns in a spreadsheet. In reality, they stack on top of each other, multiplying the danger exponentially until the pancreas simply cannot compensate further.
The Cigarette Multiplier Effect
Smoking is universally recognized as bad for the lungs, yet its profound impact on the abdomen is routinely ignored by the public. Nicotine alters pancreatic blood flow and accelerates the calcification of tissue. If you drink heavily, you have a baseline risk; if you drink heavily and smoke a pack a day, your risk of developing chronic pancreatitis doesn't just double—it jumps by a factor of four. Tobacco smoke acts as an independent accelerator, transforming mild, subclinical tissue stress into full-blown necrosis, which explains why smoking cessation is now considered a mandatory therapeutic intervention in modern GI clinics.
The Inflammatory Baseline of Excess Adiposity
Obesity changes the entire chemical baseline of the human body. Visceral fat surrounding the abdominal organs isn't inert cushioning; it functions as an active endocrine organ, pumping out a continuous stream of pro-inflammatory cytokines like interleukin-6. Consequently, an obese patient who develops a gallstone-induced attack faces a vastly higher probability of developing severe complications, such as pancreatic pseudocysts or systemic organ failure, because their baseline immune state is already primed for an overreaction. It is not just about the structural mechanics of a blocked duct anymore—it is about the systemic environment in which that blockage occurs.
Common mistakes and dangerous misconceptions
The myth of the exclusive alcohol connection
Mention the word pancreatitis to most people, and they immediately picture a heavy drinker. Let's be clear: alcohol abuse is undeniably a massive trigger, but focusing solely on it leaves millions vulnerable. The problem is that biliary issues, specifically gallstones, block the pancreatic duct just as frequently, sparking acute, life-threatening inflammation. When a person with a pristine lifestyle suffers from agonizing upper abdominal pain, they often delay seeking emergency care because they believe they are not the type who is more prone to pancreatitis. This stereotype kills. Your pancreas does not care about your moral superiority, nor does it check your bar tab before it fails.
Ignoring the silent, genetic clock
Another catastrophic error is assuming that normal blood work at age thirty means you are safe for life. Idiopathic cases account for roughly twenty percent of diagnoses, baffling traditional clinicians who refuse to look at hereditary blueprints. (Genetic testing rarely enters the standard ER protocol, which is a massive oversight). Because mutations in the SPINK1 or CFTR genes can remain dormant for decades, a sudden flare-up seems random. Yet, it is merely the inevitable conclusion of a biological countdown. Do not mistake a current lack of symptoms for permanent immunity, especially if your family history contains vague tales of chronic stomach trouble.
The trap of the quick-fix detox diet
But what about the wellness crowd? They often believe that a green juice cleanse will magically reset a sluggish digestive system. This is pure delusion. Forcing a sudden influx of raw, concentrated nutrients or undergoing extreme fasting can actually trigger acute attacks in individuals susceptible to pancreatic inflammation by violently altering gallbladder motility. Sudden dietary shifts put immense mechanical stress on the biliary tree. As a result: an organ already teetering on the edge of dysfunction gets pushed directly into a full-blown necrotizing crisis.
The hidden threat: Medication-induced vulnerability
Your medicine cabinet might be the culprit
Medical professionals frequently overlook drug-induced pancreatic injury, viewing it as a statistical anomaly. It is not. Over five hundred common medications, ranging from routine blood pressure pills like ACE inhibitors to common antibiotics like tetracycline, are actively linked to organ swelling. The issue remains that patients are rarely warned about these metabolic side effects when handed a new prescription. Why does this matter? Because a sixty-year-old managing hypertension might suddenly find themselves at higher risk for pancreatitis simply due to their daily pharmaceutical regimen. Except that instead of reviewing the drug list, doctors often spend days hunting for non-existent gallstones while the tissue continues to self-digest.
Frequently Asked Questions
Does gender dictate who is more prone to pancreatitis?
Demographic data reveals a stark, fascinating split in how this illness targets the human body based on sex. Men are statistically twice as likely to develop alcohol-induced chronic inflammation, a trend tied closely to global consumption patterns. Conversely, women experience acute episodes at a 35% higher rate due to their significantly elevated prevalence of cholesterol gallstones. Estrogen naturally increases cholesterol secretion into bile, which explains why pregnancy and hormone replacement therapy drastically accelerate stone formation. In short, your biological sex does not grant immunity; it merely changes the weapon the disease uses against you.
Can young children actually suffer from this adult disease?
Pediatric cases are rising at an alarming rate, completely dismantling the outdated belief that this is solely a disease of aging or excess. Recent epidemiological tracking indicates that pediatric incidence has surged to approximately 10 cases per 100,000 children annually, a number matching historical adult rates. Instead of lifestyle factors, these young patients are usually victims of blunt abdominal trauma from bicycle accidents, severe systemic viral infections, or congenital structural anomalies like pancreas divisum. Diagnosis is frequently delayed because pediatricians mistake the screaming child's agony for simple gastroenteritis or appendicitis. Is it not terrifying that a minor playground tumble could silently trigger a major pancreatic catastrophe?
What survival rate can a patient expect after a severe attack?
The prognosis varies wildly based on whether the tissue undergoes interstitial swelling or enters the catastrophic realm of necrotizing destruction. Mild acute episodes carry a reassuringly low mortality rate of under 1% with proper hydration and bowel rest. However, when pancreatic tissue dies and becomes infected, mortality rates aggressively skyrocket to between 20% and 30% despite modern intensive care interventions. Long-term survivors face a grueling road, as roughly 40% of these individuals subsequently develop exocrine pancreatic insufficiency or type 3c diabetes. This permanent metabolic shift requires lifelong enzyme replacement therapy and precise glucose management.
An aggressive stance on pancreatic health
We need to stop treating pancreatic health as an afterthought or a niche concern for the medically fragile. The current reactive healthcare model, which waits for a patient to double over in agonizing pain before investigating their metabolic profile, is an absolute failure. Ignorance is the primary driver of these rising hospitalization numbers. We must demand comprehensive screening that evaluates genetic risks, pharmaceutical side effects, and biliary health simultaneously. If you possess multiple risk factors, sitting around waiting for symptoms to manifest is a form of physiological roulette. Your pancreas is an unforgiving organ; once it turns its digestive enzymes inward, it does not negotiate.