Here’s the thing: a diagnosis of blocked leg arteries often feels like a life sentence of stiffness, fatigue, and doctor visits. You get scanned, you see the narrowing in the arteries, and the immediate assumption is surgery or stents. But what if the most effective tool wasn’t in a catheter lab—but on a sidewalk?
Understanding Blocked Arteries in the Legs: The Basics of Peripheral Artery Disease
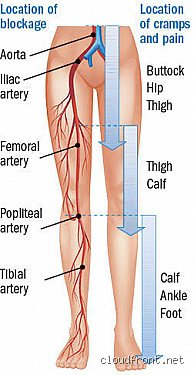
Peripheral artery disease isn’t rare. It affects about 8.5 million people in the United States alone—roughly 1 in every 12 adults over 40. And that number jumps to 1 in 5 for those over 70. The core issue? Atherosclerosis. Plaque—made of cholesterol, calcium, and cellular debris—builds up inside the arteries, especially in the legs. This narrowing reduces blood flow. Less oxygen-rich blood reaches the muscles. And that’s when the pain starts.
But PAD isn’t just about discomfort. It’s a red flag. If your leg arteries are blocked, chances are your heart or brain vessels are at risk too. In fact, someone with PAD is 5 times more likely to have a heart attack or stroke.
What Causes Arterial Blockages in the Legs?
Smoking is the heavyweight champion of risk factors—doubling or even tripling your odds. Diabetes runs a close second. High blood pressure, high cholesterol, and a sedentary lifestyle pile on. Genetics play a role, but not as much as people think. It’s lifestyle that tilts the scale. And here’s a twist: some people with severe blockages have no symptoms. Others with mild narrowing are barely able to walk a block. That’s the frustrating unpredictability of PAD.
How Do You Know If You Have It?
The classic sign is claudication—cramping, aching, or fatigue in the calf, thigh, or hip that comes on with walking and fades with rest. It’s not arthritis. It’s not aging. It’s your muscles screaming for oxygen. Yet, studies show only 25% of patients with these symptoms actually get diagnosed. Many chalk it up to getting older. That changes everything—because early action can alter the course.
How Walking Improves Blood Flow in Damaged Arteries
Walking isn’t just exercise for PAD—it’s therapy. It forces the body to adapt. When your leg muscles work under low-oxygen conditions, they signal for help. New, tiny blood vessels form. Collateral circulation kicks in. It’s like building detours around a roadblock. And the more you walk, the better those detours become.
In clinical trials, supervised walking programs increased pain-free walking distance by an average of 150%—some patients went from limping 200 meters to striding 600 meters without stopping. That’s not trivial. That’s independence. That’s being able to get to the mailbox, walk the dog, or keep up with a grandchild.
But—and this is where it gets tricky—most people don’t walk correctly for PAD. They stop at the first twinge of pain. They wait until it fades completely before starting again. That’s not how it works. The pain, within reason, is the point. You have to walk into it, rest briefly, then go again. It’s uncomfortable. That’s the design.
The Science Behind Exercise-Induced Angiogenesis
Angiogenesis—growth of new blood vessels—isn’t magic. It’s biology. Mechanical stress from muscle contraction, combined with low oxygen and increased metabolic demand, triggers the release of growth factors like VEGF (vascular endothelial growth factor). These molecules act like construction managers, directing the formation of microvessels. Over weeks, these networks become efficient enough to bypass blocked arteries to some degree. It’s a slow process, but real. And yes, it can be measured—not just in meters walked, but in ankle-brachial index (ABI) improvements. Some studies show ABI gains of 0.10–0.15 points with consistent walking, which may not sound like much, but in vascular terms, that’s significant.
How Much Walking Is Actually Needed?
The gold standard is 30 to 45 minutes of walking, 3 to 5 times a week. You don’t have to be pain-free. In fact, aim for moderate discomfort—about a 3 to 4 on a scale of 5—during each session. Rest for 1 to 2 minutes, then resume. Repeat until time’s up. It’s not enjoyable. But it works. Supervised programs show better adherence and results—patients improve 50% faster than those walking on their own. But they cost money—$30 to $60 per session, not always covered by insurance. That’s a barrier. We’re far from it being accessible to all.
Walking vs. Medical or Surgical Interventions: What Really Works?
Let’s be clear about this: walking isn’t a replacement for stents or surgery in severe cases. If you have critical limb ischemia—rest pain, non-healing ulcers, gangrene—exercise won’t save the limb. You need revascularization. But for the vast majority with mild to moderate PAD? Walking performs surprisingly well against high-tech fixes.
A 2019 JAMA study compared stent placement plus standard care to supervised walking plus standard care. After 12 months, there was no meaningful difference in walking distance between the two groups. None. The stent group spent thousands more, faced procedural risks, and took longer to recover. The walkers? They improved just as much—for free. That’s not to say stents are useless. They have their place. But they’re overused. And that’s exactly where walking gets overlooked.
Angioplasty and Stents: Fast Fix, Fading Results?
Stents open blocked arteries—no question. But restenosis (re-narrowing) happens in up to 50% of cases within a year, especially in diabetics or those with long blockages. And the procedure carries risks: blood clots, vessel tearing, or kidney damage from contrast dye. Plus, you still need to walk afterward. Otherwise, the benefits vanish. So why jump to stents when walking alone can achieve similar outcomes without a single incision?
Medication Alone Isn’t Enough
Statins, blood thinners, and drugs like cilostazol help—no doubt. Cilostazol, for instance, can boost walking distance by 30% to 50%. But it has side effects: headaches, palpitations, and GI upset. And it costs about $150 a month. Combine it with walking? Then you see real gains. But medication without lifestyle change? That’s like bailing water from a sinking boat without plugging the hole.
Practical Tips to Start a Walking Routine with PAD
You don’t need special gear. Just shoes with good support and a flat, safe route. Start slow—10 minutes a day, even if you stop every 2 minutes. Use pain as a guide, not a stop sign. Walk until it hits a 3 or 4, rest, repeat. Track your progress. Keep a log. Seeing improvement—even from 150 to 180 meters—is motivating.
Warm up for 5 minutes. Cool down for 5. That reduces injury risk. Do it at the same time each day. Routine matters. And tell your doctor what you’re doing. They might adjust your meds or order a follow-up ABI test.
One patient I followed—a retired teacher from Portland—started at 90 meters. After 12 weeks of daily walks, she hit 500. No stents. No drugs beyond aspirin. Just persistence. That’s the power of movement.
Frequently Asked Questions
Can walking worsen blocked arteries?
No. Walking doesn’t damage arteries or increase plaque. It may cause temporary pain, but that’s not harm—it’s adaptation. In rare cases of critical limb ischemia, excessive walking could delay needed care. But for most? It’s safe. Always check with your doctor first, especially if you have heart disease.
How long before I see results?
Most people notice changes in 4 to 6 weeks. By 12 weeks, improvements are usually measurable. But it’s not linear. Some weeks feel worse. That’s normal. Consistency beats intensity every time.
Is it safe to walk outside with PAD?
Yes—as long as conditions aren’t extreme. Avoid icy sidewalks, steep hills, or blistering heat. Treadmills offer controlled environments, but sidewalks, parks, or malls work too. Just stay consistent. And bring water. Dehydration thickens blood. Not ideal.
The Bottom Line
Walking is not a miracle. But it’s one of the most effective, underused treatments for blocked arteries in the legs. It beats pills in long-term outcomes, rivals stents in function, and costs nothing. The irony? The solution is something we all know how to do—yet so few actually do it. Experts disagree on how aggressively to intervene medically, but they agree on this: movement is medicine. So put on your shoes. Step outside. Walk into the discomfort. Because sometimes, the best therapy isn’t found in a clinic—it’s measured in steps.