You know that moment when someone trails off mid-sentence, searching for a word they used to know instantly? We all do it. But when it happens daily, then hourly, and the person starts substituting “thing” for everything—even “spoon” or “daughter”—that’s not normal aging. That’s something else. And that’s exactly where PPA enters the picture.
Understanding PPA: More Than Just Trouble Finding Words
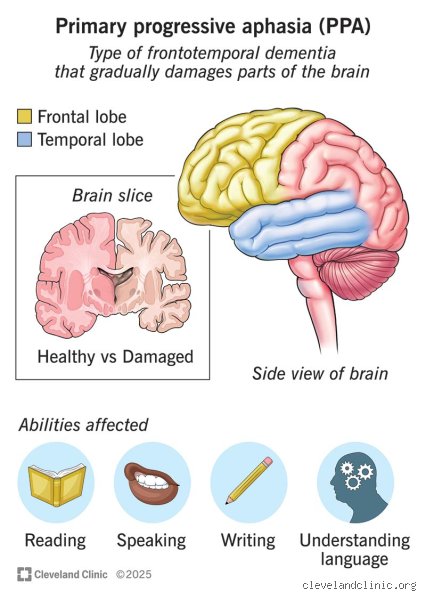
Primary progressive aphasia isn’t a sudden stroke or a temporary speech issue. It’s a slow, degenerative condition that targets the brain’s language centers—mainly in the left hemisphere. Most cases begin between ages 50 and 70, which makes it especially jarring. These aren’t elderly patients with a lifetime of wear and tear; they’re often parents, professionals, even writers and teachers whose identities are tied to communication.
And that’s where conventional wisdom starts to falter. Because when we think “dementia,” we picture someone forgetting their grandchildren’s names. But in PPA, the person may recall every birthday, every vacation, every childhood pet—yet struggle to say “I love you” out loud.
What Exactly Is Primary Progressive Aphasia?
PPA is a clinical syndrome, not a single disease. It’s caused by underlying neurodegenerative processes—most commonly frontotemporal lobar degeneration (FTLD), though Alzheimer’s pathology can also be responsible in about 30% of cases. Unlike typical Alzheimer’s, which hits memory first, PPA zeroes in on speech and language. There are three main variants: non-fluent/agrammatic, semantic, and logopenic. Each wrecks language in a different way.
In the non-fluent type, speech becomes effortful, halting, like wading through mental mud. Grammar erodes. The person might say “Walk… dog… yesterday?” instead of a full sentence. The semantic variant is eerier: fluency remains, but meaning vanishes. A “dog” becomes “animal,” then “thing,” then nothing at all. The logopenic form? That’s the struggle to retrieve words, even common ones, with frequent pauses and circumlocutions—“you know, the thing you write with” instead of “pen.”
How PPA Differs from Typical Dementia Patterns
Let’s be clear about this: calling PPA a “language disorder” undersells its impact. It’s not just about speech. People with PPA often retain self-awareness longer than those with Alzheimer’s. They know something is wrong. They feel the loss. That emotional toll is brutal. But socially? They’re often dismissed as “slow” or “rude” when they interrupt or talk over others—not because they’re impolite, but because they’re racing to get words out before they disappear.
Meanwhile, memory, reasoning, and spatial skills can remain intact for years. Which explains why some patients are misdiagnosed with depression, anxiety, or even schizophrenia. One study from Northwestern University found that nearly half of PPA patients were initially misdiagnosed. That changes everything—treatment, support, prognosis.
The Dementia Question: Why Classification Matters
Here’s the knot we keep circling: if dementia is defined by progressive cognitive decline that interferes with daily life, then yes—PPA qualifies. Full stop. But the public image of dementia is so narrow, so tied to memory loss, that calling PPA a form of dementia feels misleading to some families. And that’s fair. Perception matters. But medically? The evidence is clear.
Autopsies show brain atrophy in language regions. PET scans reveal hypometabolism. Biomarkers align with known neurodegenerative diseases. In short, this isn’t stress. It isn’t burnout. It’s brain degeneration. And when the damage spreads—which it eventually does—to memory, behavior, or motor function, the line blurs entirely.
The Neurological Overlap Between PPA and Other Dementias
PPA isn’t an island. It’s connected. About 60% of non-fluent PPA cases progress to features of behavioral variant frontotemporal dementia (bvFTD), where personality shifts, impulsivity, and emotional blunting emerge. Semantic variant PPA often evolves into semantic dementia, with object recognition problems and loss of conceptual knowledge. Logopenic PPA? More likely to transform into typical Alzheimer’s, with memory decline joining the language breakdown.
So while PPA starts focused, it rarely stays that way. A study published in Brain in 2020 followed 117 PPA patients over five years. By year four, 73% had developed additional cognitive deficits beyond language. That’s not a side effect. That’s dementia progression.
Diagnostic Criteria and the Role of Biomarkers
Diagnosing PPA requires more than a memory test. Standard cognitive screens like the MMSE (Mini-Mental State Examination) often miss it completely—scores can stay normal for years. Instead, specialists use language-specific assessments: the BDAE (Boston Diagnostic Aphasia Examination), picture naming tests, narrative analysis. MRI scans look for asymmetric atrophy in the left frontal or temporal lobes. Amyloid PET scans help determine if Alzheimer’s is the underlying cause.
But access is spotty. Many neurologists aren’t trained in aphasia subtypes. Rural clinics lack advanced imaging. And insurance? Don’t get me started. A 2023 report from the Association for Frontotemporal Degeneration found that patients wait an average of 3.7 years for a correct diagnosis. Three years of confusion. Three years of lost time.
PPA vs Alzheimer’s: A Closer Look at the Differences and Overlaps
Comparing PPA and Alzheimer’s is a bit like comparing a sniper to a bomb. Alzheimer’s is widespread—it detonates across the brain, hitting memory, orientation, judgment, and eventually language. PPA is surgical. It isolates one function and dismantles it piece by piece. But the ammunition? Often the same. Amyloid plaques, tau tangles, TDP-43 protein aggregates—they’re found in both.
Yet, the clinical path diverges. Alzheimer’s patients may forget they have an appointment. PPA patients remember the appointment but can’t call to confirm it. Alzheimer’s erases the past. PPA distorts expression. And because of that, families often don’t recognize PPA as “real” dementia until much later.
Symptom Onset and Progression Patterns
In Alzheimer’s, memory slips early—repeating questions, getting lost in familiar places. In PPA, memory holds. But communication frays. A teacher might stop grading essays. A lawyer might quit court appearances. These aren’t career burnout; they’re surrender to a crumbling linguistic world.
Progression varies. Some patients live 12 years post-diagnosis. Others decline faster. A 2018 study at UC San Francisco tracked progression speed across variants: semantic PPA advanced slower (median 10.2 years to full dependency) than non-fluent (7.4 years). Why? Unclear. Maybe because semantic loss is more gradual. Or maybe we’re far from understanding the full picture.
Underlying Brain Pathology: Shared Mechanisms?
Here’s where it gets wild: two people with identical PPA symptoms can have completely different brain pathologies. One might have FTLD-tau, another FTLD-TDP, another Alzheimer’s. And you can’t tell which without a biopsy or autopsy. That explains why drug trials fail. A treatment targeting amyloid won’t help someone whose disease is driven by TDP-43.
This is the frontier. We’re trying to match biology to behavior. But we’re not there yet. Honestly, it is unclear how many subtypes exist. Researchers at Mayo Clinic recently proposed splitting PPA into five clinical-biological categories. That’s progress. But it also means yesterday’s diagnosis might be obsolete tomorrow.
Frequently Asked Questions
Can PPA Be Reversed or Stopped?
No. There is no cure. No approved drugs slow PPA’s progression. Speech therapy helps patients adapt—using communication boards, apps, or gestures—but it doesn’t halt brain degeneration. Some trials are testing monoclonal antibodies, especially in logopenic cases with Alzheimer’s pathology. Early results? Mixed. One phase II trial showed slight delay in decline at 18 months, but only in patients with low baseline amyloid. We’re not close to a breakthrough.
Is PPA Hereditary?
Sometimes. About 10–15% of PPA cases have a strong family history. Mutations in genes like MAPT, GRN, or C9ORF72 can predispose someone, especially in non-fluent or semantic variants. But most cases are sporadic. Genetic testing isn’t routine—unless there’s a family pattern. And even then, it’s a personal choice. Because what do you do with that knowledge? That’s another conversation.
How Is PPA Treated in Daily Life?
Treatment is about adaptation. Speech-language pathologists teach strategies: writing key words, using voice-output devices, training caregivers in supported conversation. Some patients benefit from transcranial magnetic stimulation (TMS), though evidence is thin—just 3 small studies, with sample sizes under 20. More promising? Social support groups. A 2022 study found participants reported better mood and communication confidence, even without cognitive improvement. Mental health matters. Burnout among caregivers is real—divorce rates in PPA families are 40% higher than average.
The Bottom Line: PPA Is Dementia—Just Not the Kind You Expect
I am convinced that PPA belongs under the dementia umbrella. Not because it fits a stereotype, but because it meets the clinical definition: progressive, disabling, neurodegenerative. But we need better language—literally—to explain it. Calling it “just” a speech problem is like calling a hurricane “a bit of wind.”
We should stop measuring dementia by memory alone. That outdated lens leaves PPA patients in the shadows. They’re not forgetful. They’re silenced. And while research lags, families adapt in real time—learning to listen differently, to value silence, to find connection beyond words.
My advice? If someone in your life is losing language faster than they should, push for a specialist. A neurologist who knows aphasia. An academic center with imaging and expertise. Don’t accept “it’s stress.” Don’t wait. Because early intervention won’t stop PPA—but it can preserve dignity, communication, and time.
And maybe, just maybe, that’s the most human thing we can offer.