The Hidden Reality of the Pancreas and Why It Ignites
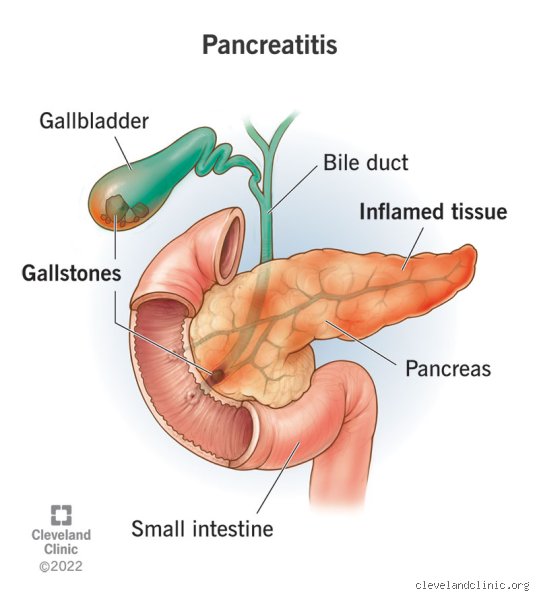
People don’t think about this enough: a tiny organ tucked behind your stomach holds enough digestive power to essentially liquefy your internal tissues if things go sideways. That is the brutal reality of the pancreas. Under normal conditions, this pale, six-inch gland functions with quiet efficiency, churning out insulin to regulate your blood sugar and synthesizing inactive enzymes that only wake up once they reach the duodenum. Except that when pancreatitis strikes, the system fails spectacularly.
When Enzymes Turn Against Their Maker
The core pathology hinges on premature enzyme activation. Imagine a factory where the products accidentally assemble themselves on the warehouse floor instead of the shipping dock. Inside an inflamed pancreas, trypsinogen transforms into active trypsin far too early, triggering a cascading nightmare of auto-digestion. I have seen how quickly this biochemical wildfire can spread, and frankly, it is terrifying. The surrounding tissues become inflamed, blood vessels leak, and the organ literally begins to digest itself. Yet, the severity of this response is a massive spectrum. It ranges from mild interstitial edema—where the organ is merely swollen and angry—to necrotizing pancreatitis, a catastrophic state where large portions of the tissue actually die. In short, the biological stakes could not be higher.
The Two Faces of Inflammation: Acute versus Chronic
We must separate the sudden explosion from the slow burn. Acute pancreatitis is an abrupt, thunderous event, often triggered by a stray gallstone blocking the pancreatic duct or a sudden surge of triglycerides after a heavy night of drinking. It hits like a sledgehammer. Chronic pancreatitis, by contrast, is a stubborn, irreversible rewriting of the organ's architecture. Over years of alcohol use, genetic anomalies, or autoimmune attacks, healthy tissue gets replaced by tough, fibrous scar tissue. Why does this distinction matter for our main question? Because a flare-up of chronic disease behaves very differently than a first-time acute attack, which explains why their respective hospitalization tracks look nothing alike.
The Triage Crisis: Deciding Who Stays and Who Goes Home
Where it gets tricky is the ER waiting room. Doctors cannot simply look at a patient doubling over in pain and instantly know if their pancreas is merely irritated or actively dying. For decades, the knee-jerk reaction was simple: admit everyone. But that changes everything when you look at modern hospital capacity and the risks of nosocomial infections. Today, physicians rely on complex scoring systems to separate the mild from the potentially fatal.
Cracking the Code of the Atlanta Classification
The medical community relies heavily on the revised Atlanta Classification system to standardize how we talk about severity. This framework divides cases into mild, moderately severe, and severe acute pancreatitis. Mild cases, which thankfully make up about 80 percent of all admissions, feature no organ failure and no local complications like fluid collections. This is the exact demographic where the question of skipping the hospital ward altogether becomes a serious conversation. Moderately severe cases involve transient organ failure that resolves within 48 hours, while severe cases mean persistent organ failure that can spiral into systemic inflammatory response syndrome (SIRS).
The Numbers Game: Ranson Criteria and the BISAP Score
To predict which way a patient will trend, emergency rooms utilize predictive scoring models. The classic Ranson Criteria, developed back in 1974, evaluates five specific parameters at admission—including an age over 55 and a white blood cell count exceeding 16,000 cells per microliter—and then checks another six metrics 48 hours later. But waiting two days for a score is a luxury ER doctors don't have. Enter the BISAP score (Bedside Index for Severity in Acute Pancreatitis). By tracking just five straightforward variables, such as a blood urea nitrogen (BUN) level over 25 milligrams per deciliter and the presence of pleural effusion, clinicians can spot high-risk patients within hours. If your BISAP score is zero or one, your statistical risk of mortality is less than one percent. Hence, the push for outpatient care gains massive scientific backing.
Redefining Mild Cases: The Blueprint for Safe At-Home Recovery
If we accept that a fifth of these patients might not need a hospital bed, what does safe home management actually look like? It is not as simple as taking a few painkillers and lying on the couch. The thing is, home care requires a meticulous alignment of specific patient factors, a reliable support network, and an incredibly compliant patient.
The Non-Negotiable Checklist for Outpatient Selection
To even be considered for home monitoring, a patient must clear a very high bar. First, they must be able to keep fluids down. Period. If constant vomiting prevents oral hydration, home care is dead on arrival. Second, their pain must be manageable with oral medications rather than intravenous narcotics. Third, they need normal vital signs—no racing pulse, no crashing blood pressure, and no raging fever. But the physical metrics are only half the battle. Does the patient live alone? Do they have a car to get back to the clinic if things take a turn for the worse? Can they comprehend the warning signs of worsening necrosis? If the answer to any of these is no, the hospital door swings open.
The Pillars of the At-Home Protocol
For the lucky few who qualify, the treatment regimen mirrors what would happen in a standard hospital room, minus the annoying alarms and the terrible food. The historic rule of "nil per os" (nothing by mouth) has been thoroughly debunked for mild cases; we now know that early oral feeding keeps the gut barrier intact and prevents bacterial translocation. Patients are started on a low-fat, soft diet almost immediately. Hydration is the next obsession. Sip water, sports drinks, or clear broths continuously. Pain management typically avoids heavy opioids, relying instead on scheduled non-opioid analgesics or short courses of tramadol. It is a delicate balancing act, yet when done right, it works beautifully.
The Hospitalization Divide: Standard Ward versus Home Care
To understand why keeping certain patients home is such a radical shift, we have to look at what traditional hospitalization actually entails. The contrast is stark, and honestly, experts disagree on exactly where the boundary line should sit for borderline cases.
What a Hospital Ward Offers That Your Living Room Cannot
The inside of a hospital offers one massive advantage: immediate intervention. When a patient is admitted for acute pancreatitis, they are hooked up to aggressive intravenous fluid resuscitation, often receiving 250 to 500 milliliters per hour of Lactated Ringer's solution. This intense hydration is critical to maintain microcirculation in the pancreas and prevent tissue necrosis. Furthermore, a hospital ward offers continuous pulse oximetry, frequent blood draws to monitor hematocrit and electrolyte shifts, and instant access to advanced imaging like contrast-enhanced computed tomography (CECT) scans if the clinical picture deteriorates. You cannot replicate that level of surveillance on your sofa.
The Hidden Toll of Unnecessary Admissions
But hospitalization is far from a benign vacation. Beyond the staggering financial burden—where a typical acute pancreatitis stay in the United States can easily exceed ten thousand dollars—the hospital environment carries inherent risks. Sleep deprivation from hourly vitals degrades immune function. Central lines and urinary catheters introduce pathways for multi-drug resistant bacteria. There is also the psychological toll of being confined to a bed, which can exacerbate anxiety and depression in chronic sufferers. We are far from suggesting that severe cases avoid the hospital, but for an uncomplicated flare-up of known chronic pancreatitis? Forcing that patient into an ER bay might actually do more harm than good.
Common Misconceptions Surrounding Pancreatic Inflammation
The internet propagates a dangerous myth: every single instance of pancreatic irritation demands an immediate, weeks-long residency in a sterile medical ward. Let's be clear, reality refuses to conform to such neat, binary boxes. While acute episodes frequently dictate emergency admissions, the landscape of chronic gland dysfunction operates under entirely separate medical architecture. Thinking that does pancreatitis always require hospitalization is a massive oversimplification that fails to account for outpatient management protocols.
The Blanket Severity Trap
Society views the pancreas as a fragile, volatile ticking time bomb. This perspective convinces people that any diagnostic whisper of inflammation equals immediate structural catastrophe. Except that physicians now utilize nuanced scoring metrics like the Ranson Criteria or the BISAP score to determine actual physiological threat levels. Mild biliary irritation often resolves rapidly once the initiating trigger—such as microscopic biliary sludge—passes naturally. Over-hospitalizing these low-risk, ambulatory individuals introduces unnecessary exposure to nosocomial infections and drives up healthcare expenditure needlessly. Do we really want to occupy a scarce intensive care bed for a patient whose localized discomfort can be remedied safely with oral hydration and temporary dietary modification at home?
The Chronic Versus Acute Mix-up
Confusion reigns supreme when patients blur the lines between an isolated, explosive flare-up and a long-standing, fibrotic disease process. An acute attack features searing, back-radiating epigastric agony, forcing an immediate trip to the emergency room due to the threat of systemic inflammatory response syndrome. Conversely, individuals navigating permanent, calcified tissue degradation experience frequent, dull, grumbling discomfort. These veterans of the disease routinely handle their symptom fluctuations in consultation with a trusted gastroenterologist. They adjust pancreatic enzyme replacement therapies, tweak low-fat nutritional regimens, and utilize targeted analgesics right from their own living rooms. Which explains why a seasoned chronic patient might avoid the clinical ward for years despite ongoing, documented organ damage.
The Hidden Biological Variable: Fluid Sequestration
Shifting focus away from sheer pain metrics reveals a stealthy pathological mechanism that truly determines whether a hospital bed bears your name: third-spacing. When the pancreas undergoes autodigestion, inflammatory cytokines compromise vascular permeability. Blood vessels leak vital plasma into the peritoneal cavity, draining the circulatory system of essential volume. This hidden fluid shift is why pancreatic inflammation clinical management focuses so heavily on aggressive intravenous resuscitation within the initial twenty-four hours.
Microvascular Collapse and Home Care Limits
You cannot drink enough water to compensate for this interior vascular drain. Trying to manage severe intravascular volume depletion via oral hydration fails because the gastrointestinal tract simply cannot absorb fluids rapidly enough during an active inflammatory crisis. If a clinician detects a hematocrit value climbing past 44% alongside an escalating blood urea nitrogen level, outpatient care becomes an impossibility. This specific hemoconcentration signals impending pancreatic necrosis and multi-organ failure. But for a highly specific subset of stable patients showing pristine laboratory values, minimal fluid shifting, and an ability to retain oral liquids, home-based recovery remains a viable path.
Frequently Asked Questions
Can mild acute pancreatitis be safely managed at home?
Yes, selected cohorts of stable patients with mild acute pancreatitis can bypass traditional ward admission if rigorous clinical criteria are met. Data from recent clinical trials indicates that roughly 15% to 20% of acute presentations present without systemic complications, organ failure, or signs of significant fluid loss. These low-risk individuals require a reliable support network, immediate access to emergency re-evaluation, and the ability to maintain adequate oral hydration without vomiting. Gastroenterologists frequently utilize specialized scoring systems to guarantee that only individuals with a zero-mortality risk profile are selected for this non-traditional ambulatory monitoring pathway. The issue remains that any sudden escalation in pain or inability to tolerate clear liquids mandates an immediate transition to an inpatient facility for intravenous support.
What specific diagnostic numbers rule out outpatient care?
Physicians analyze specific biological thresholds to immediately terminate any consideration of home-based recovery for pancreatic conditions. A serum lipase level exceeding three times the upper limit of normal establishes the diagnosis, but secondary markers like a C-reactive protein value surpassing 150 mg/L after forty-eight hours serve as a definitive indicator of severe tissue necrosis. Furthermore, any blood urea nitrogen reading that climbs consistently during initial evaluation predicts elevated mortality rates and demands continuous intravenous hydration. And because a rising hematocrit percentage signifies extreme, hidden fluid loss into the abdomen, clinicians consider an initial reading over 44% an absolute contraindication to outpatient care. These precise parameters provide an objective boundary line that safeguards vulnerable individuals from catastrophic home management failures.
How does chronic pancreatic disease alter admission requirements?
Living with permanent organ scarring fundamentally alters the clinical calculus regarding whether does pancreatitis always require hospitalization for recurrent symptom spikes. Statistics reveal that nearly 45% of individuals suffering from chronic calcifying disease experience episodic flare-ups that are successfully managed through outpatient interventions. These interventions rely heavily on adjusting oral pancreatic enzyme supplements, utilizing specialized nerve-pain modulators, and implementing strict dietary restrictions during periods of increased discomfort. Hospital admission for this demographic is typically reserved for severe complications such as a blocking pseudocyst, profound malnutrition requiring feeding tubes, or intractable vomiting that prevents the absorption of necessary medications. As a result: routine, low-grade discomfort is handled through scheduled outpatient specialist appointments rather than disruptive emergency room visits.
A Definitive Stance on Pancreatic Care
We must abandon the outdated, dogmatic view that a malfunctioning pancreas automatically requires a multi-day hospital stay. The contemporary medical paradigm shifts toward individualized risk stratification, proving that a rigid, one-size-fits-all approach hurts patients and strains medical infrastructure. Yet, we cannot let the pendulum swing too far toward casual home care; the biological volatility of pancreatic necrosis requires a deeply respectful, evidence-based approach to triage. (Admittedly, predicting the exact trajectory of organ inflammation remains an imperfect science even for seasoned specialists.) If your clinical indicators show zero systemic inflammation, minimal fluid shifts, and controllable discomfort, demanding a hospital bed is counterproductive. True medical expertise lies in distinguishing a minor, self-limiting glandular hiccup from a systemic wildfire, ensuring that intense clinical resources are reserved exclusively for those standing on the precipice of organ failure. In short, the organ dictates the setting, and modern medicine finally possesses the diagnostic precision to listen accurately.