The Anatomy of Vulnerability: Demystifying Pancreatic Adenocarcinoma
The pancreas is a stubborn, dual-purpose organ hidden deep within the abdomen, split between making digestive enzymes and regulating your blood sugar. When cells in the exocrine ducts mutate, they spawn pancreatic ductal adenocarcinoma, which accounts for over 90 percent of cases. People don't think about this enough, but the organ’s deep, secluded location means a tumor can grow for months without triggering a single warning sign. Where it gets tricky is that the symptoms—vague back pain, unexplained weight loss, or mild nausea—mimic basic indigestion or aging. By the time jaundice sets in because a mass is choking the bile duct, the biological clock is already ticking loudly.
The Statistical Peak and Age Dynamics
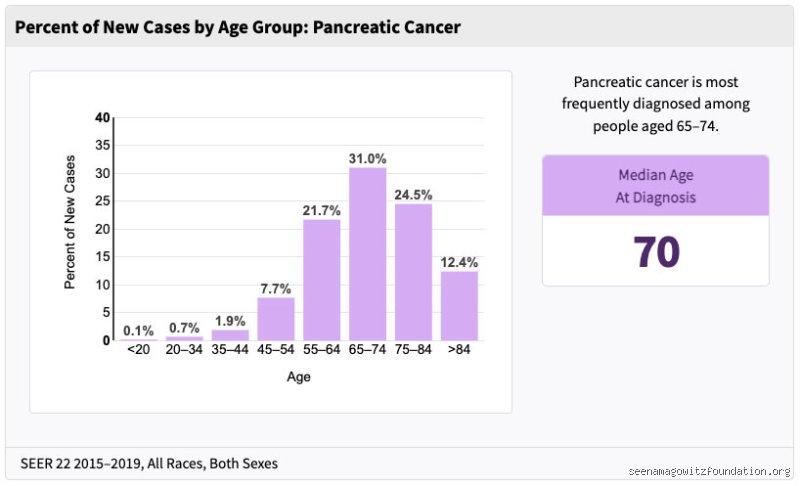
Age is the undisputed heavyweight champion of risk factors. You rarely see a diagnosis before age 45; in fact, the median age at diagnosis is 70 years old, according to data from the Surveillance, Epidemiology, and End Results (SEER) program. Why? Because cellular replication errors pile up over seven decades. But here is my hot take that contradicts conventional wisdom: while the raw numbers skew elderly, the rising incidence rate in adults under 50—particularly young women—is the real story we should be panicking about, yet mainstream oncology often brushes it off as a statistical anomaly.
The Biological Sandbox
Inside the tissue, a vicious cascade of genetic misfires takes place. It usually starts with a mutation in the KRAS oncogene, a molecular switch that gets stuck in the "on" position, forcing cells to divide like wildfire. But that changes everything when tumor suppressor genes like TP53 or CDKN2A fail alongside it. Honestly, it's unclear exactly why some pancreases tolerate these mutations for decades while others succumb rapidly, as experts disagree on the precise trigger that turns a benign cyst into a runaway freight train.
Unmasking the Primary Profiles: Age, Gender, and Ethnic Disparities
The disease does not distribute its suffering equally across the population. If you look at the raw epidemiological spreadsheets, a distinct demographic profile emerges, one shaped by genetics, systemic inequities, and biology. Men are diagnosed at a rate roughly 15 to 20 percent higher than women. This gap used to be blamed entirely on historical smoking trends—men simply smoked more forty years ago—but as smoking rates have converged, the gender gap has stubbornly refused to close entirely, which explains why researchers are now hunting for hormonal or metabolic culprits.
The Racial Gap in Oncology
The numbers regarding race are deeply unsettling. Black Americans experience an incidence rate that is up to 20 percent higher than white Americans, and they face significantly worse survival outcomes. Is it purely genetic? No, we're far from it, because socioeconomic factors, unequal access to high-volume surgical centers, and higher rates of diabetes play massive roles. Yet, specific hereditary variations cannot be ignored entirely, as certain populations show a higher baseline frequency of pre-disposing mutations.
Geographic Hotspots and the Global Picture
The thing is, pancreatic cancer is primarily a disease of Westernized, industrialized nations. The highest incidence rates are found in North America and Western Europe, specifically countries like Denmark and France, whereas parts of Central Africa show remarkably low numbers. This geographical divide points less to latitude and more to the modern lifestyle—sedentary habits, processed diets, and chemical exposures—that characterizes wealthy economies.
The Double-Edged Sword of Genetic Inheritance and Family History
Most cases are sporadic, meaning they happen by bad luck and bad habits, but roughly 10 percent of pancreatic cancers are driven by inherited genetic syndromes. If you have two or more first-degree relatives who have faced this diagnosis, your personal risk skyrockets. Think of it as inheriting a book where a crucial page has already been ripped out.
The BRCA Paradox and Other Syndromes
Most people associate the BRCA1 and BRCA2 gene mutations exclusively with breast and ovarian cancer. But did you know that carrying a BRCA2 mutation increases your risk of pancreatic cancer by up to six-fold? It is a shared flaw in the homologous recombination DNA repair pathway—a mouthful of a biological term that basically means the body loses its ability to fix broken DNA. Other culprits include Lynch syndrome, which usually causes colorectal tumors, and Familial Atypical Multiple Mole Melanoma (FAMMM) syndrome, caused by mutations in the CDKN2A gene.
The Hereditary Pancreatitis Factor
Then there is hereditary pancreatitis, a rare genetic condition where the pancreas essentially cooks itself in its own digestive juices from childhood. Individuals with this condition have a lifetime risk of developing pancreatic cancer that approaches a staggering 40 percent by age 70. Imagine living with an organ that is permanently inflamed, constantly scarring, and perpetually on the verge of malignant transformation.
Lifestyle Triggers versus Unavoidable Biology: A Comparative Breakdown
We often like to think we can out-diet or out-exercise any disease, but pancreatic cancer laughs at our hubris. It represents a complex tug-of-war between modifiable lifestyle risks and the unyielding hand of hereditary biology. Cigarette smoking is the most significant avoidable cause, responsible for about 20 to 25 percent of all pancreatic malignancies, because tobacco carcinogens enter the bloodstream and directly bathe the pancreatic tissue. If you smoke, you double your risk compared to a lifetime abstainer.
Obesity and the Insulin Connection
Obesity runs a close second to smoking, increasing risk by about 20 percent. This happens because excess adipose tissue triggers chronic, low-grade systemic inflammation while simultaneously causing insulin resistance. The pancreas responds by pumping out massive amounts of insulin, a hormone that, unfortunately, doubles as a potent growth factor for cancer cells. But the issue remains: plenty of marathon-running vegans get pancreatic cancer while lifelong smokers die of old age with a perfectly healthy pancreas. As a result: we cannot view lifestyle choices as a total guarantee of immunity, but rather as a way to tilt the odds in our favor.
The Diabetes Conundrum
Where it gets exceptionally messy is the relationship with Type 2 diabetes. New-onset diabetes in an older adult—specifically when blood sugar spikes out of nowhere after age 50 without any weight gain—is often not a lifestyle disease at all, but rather the very first symptom of a hidden tumor destroying islet cells. Is diabetes the cause or the consequence? In short, it is frequently both, a biological chicken-and-egg scenario that frustrates clinicians worldwide.
Common mistakes and misconceptions surrounding pancreatic malignancy
The "death sentence" fallacy
Receiving a diagnosis of this nature terrifies anyone. Instantly, minds drift to a grim, immediate finality. Let's be clear: while the statistics remain notoriously brutal, treating this pathology as an instant expiration date is a dangerous oversimplification. Medical advancements, particularly in neoadjuvant therapies, are shifting the goalposts. Some tumors previously deemed entirely inoperable are now being successfully resected after targeted shrinking. The problem is that public perception lags decades behind clinical realities, causing some patients to succumb to nihilism before exploring aggressive, modern interventions.
Misattributing the silent, vague warnings
Who most commonly gets pancreatic cancer? Often, it is individuals who spent months ignoring whispers from their own abdomen. People frequently chalk up persistent, dull back pain or sudden indigestion to aging or a poor diet. They self-medicate with antacids. But what happens when that nagging discomfort is actually a tumor pressing against the celiac plexus? By the time manifest jaundice or sudden-onset, non-obesity-related diabetes appears, the window for early-stage intervention has frequently slammed shut. A synchronous presentation of new-onset diabetes and unexplained weight loss in an individual over 50 demands immediate, rigorous scanning, not a casual lifestyle tweak.
Assuming it only strikes heavy smokers or drinkers
Tobacco usage undeniably doubles the risk. Yet, a clean ledger of health choices does not grant absolute immunity. Many patients walk into oncology clinics utterly bewildered because they never touched a cigarette and ran marathons. Genetics, random somatic mutations, and insidious environmental toxins play a massive, quiet role. Assuming only the stereotypical high-risk demographic gets sick leaves a vast population of ostensibly healthy adults dangerously off-guard.
The metabolic trap: A little-known expert perspective
The clandestine link to new-onset type 2 diabetes
Oncologists are increasingly focusing on a bizarre phenomenon where the pancreas effectively sabotages its own endocrine function months before a structural lump becomes visible on a standard ultrasound. For decades, scientists viewed diabetes merely as a secondary complication of a destroyed organ. Except that newer data reveals a fascinating, sinister inverse relationship: a tumor can actually secrete factors that induce profound insulin resistance. Which explains why a sudden, atypical diabetic diagnosis in a patient with no family history of metabolic syndrome is now viewed as an early warning beacon. Screening protocols must evolve to capture this cohort before traditional symptoms manifest.
Think about the sheer clinical utility of this realization. If we can track these sudden metabolic shifts in patients aged 50 to 70, we might catch the disease at a stage where surgical resection is still a viable option. It requires a radical shift in how primary care physicians view glycemic spikes in older adults (a parenthetical aside: most doctors still just prescribe metformin and move on). We cannot afford that complacency anymore.
Frequently Asked Questions
Does a family history mean you will definitely develop the disease?
Absolutely not, though it significantly elevates your baseline vulnerability. Approximately 10% of all pancreatic malignancies possess a hereditary link, often tied to mutations in the BRCA1, BRCA2, or PALB2 genes. If you have two or more first-degree relatives who suffered from this condition, your relative risk escalates up to sixfold compared to the general population. Surveillance programs utilizing endoscopic ultrasound and magnetic resonance cholangiopancreatography are specifically designed for this high-risk group to detect precancerous lesions. Is it terrifying to live with that genetic sword of Damocles hanging over your head? Naturally, but proactive surveillance allows clinicians to intervene long before a full-blown malignancy establishes its stronghold.
At what specific age does the risk peak for most populations?
Data from global registries indicates that the probability of diagnosis scales sharply after five decades of life. The median age at diagnosis sits squarely at 70 years, meaning the vast majority of cases hit during the twilight of middle age and throughout retirement. It is exceedingly rare before the age of 40, accounting for less than 1% of the total disease burden. As a result: age remains the single most potent, non-modifiable demographic risk factor that epidemiologists track. This stark reality underscores the necessity of maintaining high clinical suspicion when geriatric patients present with ambiguous abdominal complaints.
Can lifestyle changes completely eliminate your chances of diagnosis?
No lifestyle matrix offers a flawless shield against random cellular replication errors, but mitigation is entirely possible. Eliminating tobacco usage can drop your personal risk back toward baseline levels over a decade, preventing a massive chunk of avoidable cases. Maintaining a healthy body mass index also alters the systemic inflammatory environment, which is vital since obesity increases vulnerability by roughly 20%. In short, while you cannot rewrite your inherited DNA, you can actively dismantle the environmental catalysts that accelerate tumor initiation. Vigilance paired with metabolic health remains your most potent weapon.
A definitive stance on the future of detection
We must stop treating pancreatic malignancy as an unavoidable stroke of tragic cosmic bad luck. The current medical paradigm waits for patients to turn yellow before acting, a reactionary strategy that ensures dismal survival rates. True progress requires aggressive, widespread genetic and metabolic screening of the 50-to-70 age demographic exhibiting sudden glycemic instability. Waiting for perfect, risk-free screening tools is a luxury paid for in human lives. We must draw a line in the sand and demand that primary care medicine treats sudden metabolic shifts with the same urgency as a lump in a breast. Only by hunting this disease aggressively in its quietest phases will we finally break the terrifying stranglehold it has maintained on families for generations.