The Cellular Reality Behind Trisomy 21 and the Mechanics of Chance
To grasp why certain groups face higher probabilities, we have to look at what is happening inside the microscopic architecture of a developing egg. Down syndrome, known scientifically as Trisomy 21, is not typically an inherited condition passed down through family lineages. Instead, it is a blueprint error. During a process called meiosis, chromosomes are supposed to separate evenly so that an egg or sperm carries exactly 23 chromosomes. But sometimes the machinery jams. A phenomenon called nondisjunction causes chromosome pair 21 to stick together, meaning one reproductive cell ends up with an extra copy. When fertilization happens, the resulting embryo inherits three copies instead of two. I find it remarkable how a microscopic hesitation in a single cell can fundamentally alter a human life forever.
The Overlooked Subtypes: Mosaicism and Translocation
The story gets a bit messy because not all cases look identical under a microscope. While standard nondisjunction accounts for roughly 95% of all diagnoses, two other variants exist that completely scramble the traditional risk profiles. In Mosaic Down syndrome, the cellular misstep happens after fertilization during early embryonic mitosis. This means the child has a mixture of cells—some with 46 chromosomes, others with 47. Mosaicism is entirely random and unrelated to parental age, which completely contradicts the standard medical narrative. Then there is translocation, occurring in about 4% of cases, where a piece of chromosome 21 attaches itself to another chromosome, usually chromosome 14, during cell division.
When Heredity Actually Matters: The Balanced Carrier Dilemma
This is where the genetic counselors get nervous. Translocation is the only form of Down syndrome that can be inherited from a completely healthy parent. A person can walk around for decades never knowing they are a balanced translocation carrier because their genetic material is rearranged but complete. They have no physical traits of the condition. But when they try to conceive, the risk of passing on an unbalanced translocation to their offspring rises dramatically. If the mother carries the balanced translocation, the chance of having a child with Down syndrome is about 10% to 15% in every single pregnancy. If the father is the carrier, the risk drops to around 3%. Why the stark difference between maternal and paternal transmission rates? Scientists are honestly still debating the exact biological filters at play during spermatogenesis, proving that our clinical certainty has some major blind spots.
The Relentless March of Time: Maternal Age as the Primary Risk Driver
The biological clock is a phrase people throw around carelessly, yet in cytogenetics, it represents an inescapable reality. A human female is born with all the eggs she will ever possess, created while she was still a fetus in her own mother's womb. Those eggs sit in a state of suspended animation for decades, exposed to everything the woman experiences. By the time a woman reaches her late thirties, those cellular bonds—specifically the cohesin proteins that hold chromosome pairs together—begin to degrade. The machinery is simply old, making nondisjunction far more likely to occur during ovulation.
Breaking Down the Hard Probability Curve by the Numbers
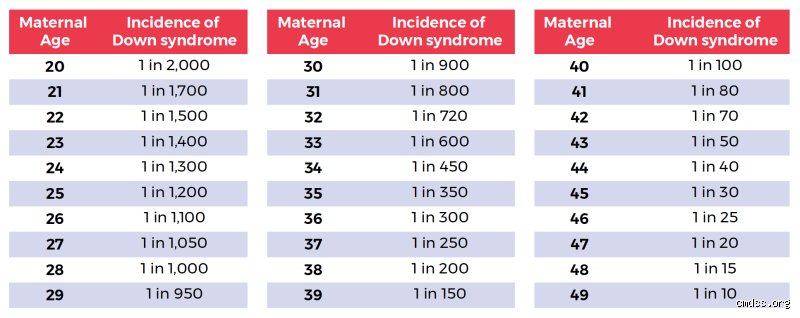
Let's look at the actual numbers because the escalation is not a gentle slope; it is a steep cliff. A 25-year-old woman has a 1 in 1,250 chance of conceiving a child with Trisomy 21. By the time that same woman celebrates her 35th birthday, her statistical probability shifts dramatically to approximately 1 in 350. The acceleration from that point onward is staggering. At age 40, the risk jumps to 1 in 100, and by age 45, it becomes a 1 in 30 reality. This is why medical communities historically branded age 35 as advanced maternal age, creating an arbitrary line in the sand that changes everything about how pregnancies are managed globally.
The Maternal Age Paradox: Why Young Mothers Give Birth to the Most Affected Infants
But here is the twist that people don't think about this enough: if older women are at the highest individual risk, why are approximately 80% of children with Down syndrome born to women under the age of 35? It sounds like a contradiction, except that it is just pure demographics. Younger women have vastly higher birth rates overall. If a massive population of women under 35 has a low-risk percentage, they will still collectively give birth to more babies with the condition than a very small population of 42-year-old women with a high-risk percentage. It is a vital distinction. It means that screening protocols focusing exclusively on older mothers miss the vast majority of cases, a systemic flaw that drove the medical industry to overhaul its entire prenatal testing strategy over the last two decades.
Paternal Contribution and Environmental Variables: Sorting Fact from Fiction
For generations, the medical establishment laid the responsibility for genetic anomalies squarely at the feet of women. We now know that historical bias skewed the data. What about the fathers? Sperm is regenerated constantly every few months, which provides some protection against the wear and tear of aging, yet the paternal factory is not entirely immune to genetic glitches.
Does Advanced Paternal Age Alter the Math?
The data regarding fathers is where it gets tricky. Research indicates that advanced paternal age does play a role, but predominantly when paired with an older maternal partner. A 50-year-old man married to a 25-year-old woman does not statistically alter the Down syndrome baseline in a significant way. However, if that same 50-year-old man is conceiving with a 40-year-old woman, his aging sperm appears to compound the existing maternal risks. Studies suggest that in a small percentage of cases, the extra chromosome 21 originates from the father, and this paternal nondisjunction correlates with men over the age of 50. The genetic replication machinery in older men simply begins to lose its precision, leading to micro-deletions and replication errors that can influence embryonic viability.
Debunking the Lifestyle and Environmental Claims
Every time a couple receives a diagnosis, the immediate, heartbreaking human reaction is to ask: What did we do wrong? People look at prenatal exposure to plastics, organic diets, smoking, prescription medications, or stressful career environments. Let us be entirely unequivocal here: no lifestyle choices, environmental toxins, or maternal behaviors have been scientifically linked to an increased risk of Down syndrome. You cannot cause Trisomy 21 by lifting heavy objects, drinking coffee before you knew you were pregnant, or living near a cell phone tower. It is an accidental chromosomal event that occurs at the very dawn of conception, completely indifferent to socioeconomic status, geographic location, or ethnic background.
Comparing Screening Accuracy: Who Faces the Highest Risk of False Positives?
Because risk profiles dictate which medical procedures a pregnant person is offered, the landscape of prenatal testing has turned into a highly sophisticated technological arms race. However, the math behind these tests depends entirely on the baseline risk of the person taking them, a nuance that many clinical providers fail to explain adequately to anxious expectant parents.
The Mathematical Trap of Non-Invasive Prenatal Testing (NIPT)
Consider the modern cell-free DNA screen, often referred to as NIPT. This test isolates fragments of placental DNA floating in the mother's bloodstream as early as week 10 of pregnancy. In a 40-year-old pregnant person, the test is incredibly predictive because the baseline prevalence of Trisomy 21 is high. If the NIPT comes back positive for a 40-year-old, there is roughly a 93% chance the fetus actually has Down syndrome. But what happens when a 22-year-old woman takes the exact same test? Because her baseline risk is so low, the Positive Predictive Value of an NIPT drops to around 50% for young mothers. That means half of the positive results given to young women are actually false alarms. This is an ironic twist: the very technology designed to give clarity often creates the most profound psychological chaos for the demographic considered to be at the lowest risk.
Common mistakes and misconceptions surrounding chromosomal risks
The myth of absolute immunity for young parents
You might think a twenty-year-old mother is entirely shielded from this genetic reality. Except that the data tells a completely different story. While the statistical probability per pregnancy is undeniably lower in youth, young women give birth to the vast majority of babies globally. Because of this massive birth volume, approximately eighty percent of children born with Down syndrome are actually delivered by mothers under thirty-five. It is a mathematical paradox that catches thousands of families off guard every year. Society fixates so intensely on geriatric pregnancies that we completely obscure the raw volume of births occurring in younger demographics.
Confusing hereditary transmission with random cellular errors
Is it running in the family? Usually, no. The issue remains that a staggering ninety-five percent of these cases arise from standard trisomy 21, which is a completely random event during meiosis. It is not an inherited trait passed down through generations like eye color or baldness. Let's be clear: a parent cannot cause this nondisjunction event through stress, diet, or minor lifestyle choices during early gestation. Only a rare variant, translocation, involving about three to four percent of cases, can be genuinely inherited from a balanced carrier parent. Yet, the average person still blames maternal behavior or a distant cousin's medical history for a completely unpredictable cellular slip-up.
The paternal factor and proactive clinical insights
Does the father's age influence genetic outcomes?
Science spent decades hyper-focusing exclusively on the maternal womb. We treated sperm as immortal, pristine vectors of genetic material. That was an oversight. Recent reproductive data indicates that advanced paternal age, specifically men over fifty, introduces its own layer of replication friction. When combined with a maternal age over forty, the paternal contribution can significantly compound the probability of a child with Down syndrome. Why did we ignore this for so long? Perhaps it was comfort, or perhaps it was just bad science. Sperm quality degrades, mutations accumulate, and the cellular machinery falters. It takes two gametes to form a zygote, after all.
Advanced screening protocols versus invasive diagnostics
Navigating modern prenatal care feels like walking through a minefield of statistics and acronyms. Today, non-invasive prenatal testing (NIPT) analyzes cell-free fetal DNA circulating directly in the maternal bloodstream as early as week ten. It boasts a 99% detection rate for trisomy 21. Which explains why older expectant parents rely heavily on it to make informed life decisions. But a screening test is not a final verdict. If a red flag appears, you must confirm the findings through amniocentesis or chorionic villus sampling (CVS). These procedures carry a slight risk of miscarriage, generally estimated around one in five hundred to one in one thousand cases, making the diagnostic journey a deeply personal calculus of risk versus certainty.
Frequently Asked Questions
What is the precise statistical probability of having a child with Down syndrome at age thirty-five versus age forty?
The statistical curve spikes dramatically during these five critical years of reproductive life. At age thirty-five, a woman faces a probability of approximately one in three hundred and fifty. By the time that same individual reaches age forty, those odds compress significantly to about one in one hundred. As a result: the biological timeline accelerates its genetic shifts with every passing year. These specific numbers represent global averages gathered across millions of live births, demonstrating how the risk profile compounds exponentially rather than linearly as maternal cell division slows down over time.
Can lifestyle modifications or specific prenatal vitamins reduce the likelihood of a child with Down syndrome?
No medical intervention, superfood diet, or prenatal vitamin regimen can alter the fundamental chromosomal alignment of an embryo once conception has occurred. Nondisjunction is a structural, mechanical error in chromosome segregation that happens as the egg or sperm is maturing. Folic acid is excellent for preventing neural tube defects like spina bifida, but it possesses zero influence over trisomy 21 development. Are we seriously still hoping a magic pill can fix a complex cellular division anomaly? The reality is that no lifestyle choice increases or decreases this specific risk, making genetic screening the only reliable window into the pregnancy's chromosomal status.
If a couple already has one child with Down syndrome, what is their statistical probability of recurrence in subsequent pregnancies?
For parents who have already navigated this journey with standard trisomy 21, the subsequent recurrence rate generally sits at roughly one percent or the age-specific risk, whichever happens to be higher. This slight elevation reflects potential underlying biological factors that current testing might not fully capture. However, if the initial child had translocation Down syndrome, the genetic landscape changes completely. In those specific scenarios, if a parent is found to be a carrier of the balanced translocation, the future recurrence probability can skyrocket to as high as ten to fifteen percent depending on which parent carries the rearranged chromosome.
A definitive perspective on reproductive genetics
We must stop treating chromosomal variations as a looming shadow or a personal failure of timing. While maternal age remains the most potent statistical predictor of who is at highest risk for having a child with Down syndrome, numbers alone are a terrible way to measure the human experience. Obsessing over percentages obscures the lived reality of families who thrive alongside their children. Information should empower future parents, not terrorize them into submission. Let's be clear: a society that truly values human life must invest as much into neurodivergent support systems as it does into advanced prenatal screening technologies. True medical progress means balancing cold, hard genetic data with radical empathy and unconditional structural support for every family, regardless of their chromosomal blueprint.