The Hidden Topography of Intracranial Growths and Why Anatomy Dictates Survival
We like to think of the brain as a uniform, mysterious mass of gray jelly, but oncologically speaking, it is a highly compartmentalized grid of real estate. The thing is, tumors do not sprout randomly like weeds in an untended garden. They have distinct, terrifying preferences. Primary brain tumors—those originating directly within the skull rather than traveling from a distant lung or breast—overwhelmingly favor the supratentorial region, which is just the medical establishment's fancy way of describing the upper vault of the skull containing the cerebral hemispheres. Meningiomas, which account for roughly 39% of all primary brain tumors according to the Central Brain Tumor Registry of the United States (CBTRUS), love the protective membranes hugging the outermost curves of the brain. But when we pivot to malignant entities like glioblastoma, the rules change entirely.
The Glial Cellular Matrix and the Frontotemporal Trap
Why do the frontal and temporal lobes bear the brunt of these cellular invasions? It comes down to sheer volume and mitotic activity. These expanses contain massive concentrations of astrocytes and oligodendrocytes, the support cells that keep our neurons firing but occasionally mutate into fast-growing gliomas. Honestly, it’s unclear why the occipital lobe at the very back of your head remains relatively spared, but the data does not lie. The frontal lobe, that massive executive suite behind your forehead responsible for your personality and impulse control, is the frequent flyer lounge for aggressive astrocytomas. But where it gets tricky is differentiating these primary residents from foreign invaders.
Tracking the Footprints of Metastatic Invaders in the Gray-White Junction
This is where we must challenge the conventional wisdom that brain tumors are mostly born inside the head. We are far from it. In fact, metastatic brain tumors—cancer that metastasized from elsewhere—outnumber primary brain tumors by a factor of at least ten to one, completely rewriting the statistical map of intracranial oncology. Every year in the United States alone, an estimated 200,000 cases of brain metastases are diagnosed, compared to roughly 90,000 primary tumors. And these opportunistic migrants do not care about the frontal lobe's architectural grandeur; they have a completely different favorite neighborhood.
The Watershed Areas and the Microvascular Bottleneck
Imagine a winding river slowing down as it branches into tiny, narrow creeks; this is precisely what happens to your blood flow at the gray-white matter junction. Cancer cells breaking away from a primary tumor in the lung (which causes about 50% of all brain metastases) or a melanoma lesion in the skin ride the arterial highway until the vessels shrink. They get stuck. This microvascular bottleneck turns the boundary zone between the brain's processing tissue (gray matter) and its wiring network (white matter) into a minefield. And because the blood supply in these watershed territories is so intricate, a single patient might present with fifteen distinct lesions scattered across both hemispheres, making surgical removal a logistical nightmare. Yet, we still treat these secondary invaders with the same urgency as native growths.
The Cerebellum and the Posterior Fossa Anomaly
But what about the back of the head? The cerebellum, that dense, cauliflower-like structure regulating your balance and motor coordination, handles about 15% of all metastatic deposits. Here, space is at an absolute premium. A tiny tumor in the cerebrum might hide silently for months without causing a peep, but a growth in the tight confines of the posterior fossa will block the flow of cerebrospinal fluid almost immediately, leading to a dangerous backup called hydrocephalus. It is a brutal spatial reality: a millimeter of growth in the wrong spot changes everything.
How Age and Pathology Completely Flip the Intracranial Map
Here is a sharp opinion that modern neuro-oncology forces us to accept, even if it contradicts the comforting narrative of standardized medicine: there is no single "most common spot" because the human brain completely remodels its oncological vulnerability as we age. If you are an adult, your tumors are almost certainly supratentorial, lurking in the vast upper plains of the cerebral cortex. But if you are looking at a pediatric patient in a children's hospital like St. Jude in Memphis, that rulebook is completely useless. In children, the script is flipped upside down, and the most common spot shifts dramatically downward into the infratentorial compartment.
The Pediatric Shift to the Brainstem and Cerebellum
Children do not get the classic frontal lobe glioblastomas of adulthood. Instead, their vulnerability clusters around the brainstem and the cerebellum, deep in the basement of the skull. Medulloblastomas and pilocytic astrocytomas dominate this space, often arising right in the middle of the cerebellum near the fourth ventricle. Even more devastating are Diffuse Intrinsic Pontine Gliomas (DIPG), which embed themselves directly into the pons—the critical bridge of the brainstem that controls breathing, heart rate, and swallowing. You cannot surgically resect a tumor that has woven itself into the very fabric of the hardware that keeps a child's heart beating, which explains the tragic prognosis associated with these specific coordinates. People don't think about this enough when discussing brain cancer; the biological behavior of a cell is intimately shackled to the age of the host environment.
Primary vs Secondary Hotspots: A Tale of Two Disparate Pathologies
To truly grasp the geography of this disease, we have to look at the stark contrast between how primary and secondary tumors claim their territory. A primary glioblastoma is a solitary, sprawling monster. It typically starts in one hemisphere, frequently the temporal lobe, and uses the corpus callosum—the thick bridge of nerve fibers connecting the two halves of the brain—like a highway to cross over into the opposite side, creating a classic "butterfly glioma" appearance on an MRI scan. It is a deeply invasive, localized occupation. Metastatic disease, by contrast, is anarchic and pluralistic.
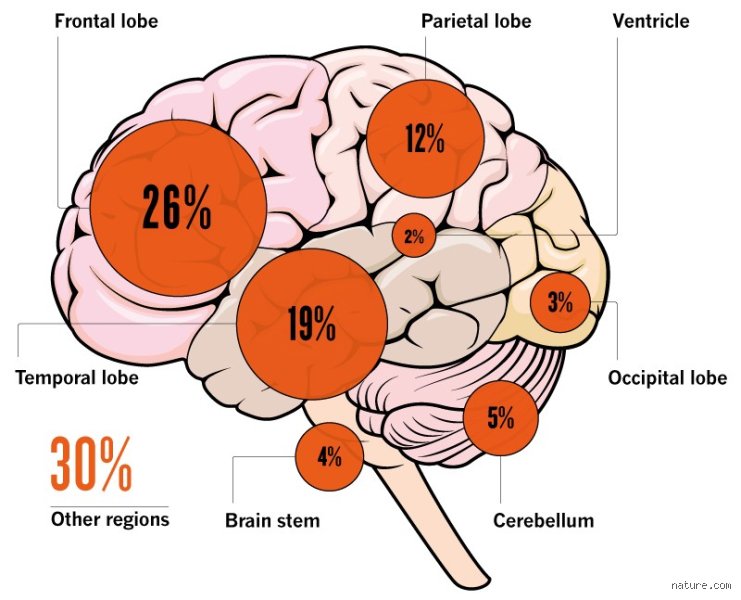
The Mathematical Reality of Tumor Distribution
Look at the hard breakdown of where these tumors actually anchor themselves across the human population. The cerebral hemispheres absorb the absolute majority of the blow, holding roughly 80% of all intracranial tumors due to their massive volume. The cerebellum takes about 15%, while the brainstem and spinal cord manage to escape with a mere 5% of the total oncological burden. But these percentages hide the human reality. A 2-centimeter meningioma sitting benignly on the parasagittal dura mater might require nothing more than a "watch and wait" approach for a decade, whereas that exact same 2-centimeter mass nestled in the speech-centers of the left frontal lobe (Broca's area) will instantly strip a person of their words, transforming an eloquent teacher into someone who can only stutter in frustration. As a result: oncologists care far less about the total volume of a tumor than they do about its precise coordinate on the map.
Common Misconceptions Surrounding Tumor Locations
The Myth of the Mobile Growth
Many patients arrive in clinics terrified that a neoplasm will migrate from one hemisphere to another overnight. It does not work that way. A primary malignancy is rooted in its tissue of origin, anchoring itself within specific anatomical boundaries. The problem is that public understanding conflates metastatic spread with physical shifting. While secondary lesions can appear in multiple areas because cells travel through the bloodstream, the original mass stays put. Why do people still believe tumors wander like loose marbles? Blame cinematic portrayals and poor internet summaries that confuse tracking a disease with tracking a physical object.
The Frontal Lobe Bias
Because cognitive shifts and personality changes grab headlines, society assumes the frontal lobe is always the culprit. It is a logical trap. True, frontally located masses trigger dramatic behavior alterations, yet statistical data paints a different picture. Meningiomas favor the sagittal sinus and sphenoid wing, while glioblastomas frequently hijack the deep white matter of the temporal and parietal regions. Let's be clear: neurological drama does not equal statistical frequency. Doctors routinely discover completely asymptomatic growths in the occipital region during routine scans for unrelated trauma, proving that the quietest zones are often the most crowded.
Benign Equals Harmless
The word benign sounds like a relief, except that location rewrites the entire medical rulebook inside a rigid skull. A non-cancerous meningioma resting on the brainstem is vastly more perilous than a low-grade glioma situated in a redundant portion of the non-dominant frontal lobe. Space is the ultimate premium. As a result: rigid histological classification matters less than anatomical real estate. When a supposedly benign growth compresses the fourth ventricle, it blocks cerebrospinal fluid flow, creating life-threatening hydrocephalus regardless of its cellular innocence.
The Hidden Impact of Microenvironment and Drainage
The Glymphatic Highway and Tumor Mapping
Neurologists are shifting their focus from simple structural geography to the complex fluid dynamics of the glymphatic system. This specialized waste-clearance network operates primarily during deep sleep, flushing metabolic debris out of the parenchyma. Experts now theorize that regions with high glymphatic traffic or altered interstitial fluid pressure might inadvertently create sanctuaries for circulating tumor cells. The issue remains that we cannot easily map these microscopic fluid currents in a living patient. (We are still relying on high-resolution contrast MRIs to see the aftermath rather than the fluid journey itself).
Surgical Accessibility vs. Biological Hotspots
Where a tumor lives dictates whether a neurosurgeon can safely resect it, creating a stark divide between operable and inoperable landscapes. The cerebral cortex offers a relatively straightforward path for surgical navigation. In contrast, deep-seated thalamic lesions or pontine gliomas present an existential challenge because every millimeter of surrounding tissue controls vital life functions. We can remove a massive growth from the right frontal pole with minimal deficit. But a tiny nodule in the brainstem? That is an entirely different conversation, which explains why geographic operability dictates long-term prognosis far more than tumor volume alone.
Frequently Asked Questions
Where is the most common spot for a brain tumor to develop in adults?
In adult populations, the cerebral hemispheres represent the most frequent site for primary brain tumors, with the frontal and temporal lobes bearing the highest statistical burden. Data from central brain tumor registries indicate that glioblastomas, the most aggressive primary entities, manifest within these lobar structures in over 60 percent of documented adult cases. Conversely, meningiomas, which account for roughly 39 percent of all primary central nervous system tumors, frequently cluster along the meningeal layers near the top of the skull. This uneven distribution means that clinicians must maintain a high index of suspicion when patients present with progressive localized headaches or focal seizures. The structural vulnerability of these specific lobes correlates tightly with their large total tissue volume relative to the rest of the intracranial space.
Does the most common spot for a brain tumor differ significantly in children?
The anatomical landscape changes drastically when transitioning from adult to pediatric oncology. In children, the most common spot for a brain tumor shifts downward into the infratentorial region, specifically the cerebellum and the brainstem. Clinical statistics show that approximately 60 percent of pediatric brain tumors originate in this posterior fossa, contrasting sharply with adult trends. Medulloblastomas and pilocytic astrocytomas dominate this space, frequently causing immediate symptoms by disrupting balance and blocking fluid pathways. This distinct geographic preference requires entirely different diagnostic and surgical approaches for young patients. Understanding this age-based anatomical inversion is vital for emergency room physicians who must evaluate children presenting with persistent morning vomiting and unsteadiness.
How do doctors determine the exact coordinates of an intracranial mass before surgery?
Neurosurgeons utilize an advanced protocol called stereotactic navigation to pinpoint the exact location of a growth prior to making an incision. This process merges high-resolution structural MRI data with functional imaging to create a highly accurate three-dimensional digital map of the patient's cranium. During this preparation, specific landmarks on the patient's face or scalp are calibrated against the digital scans, achieving an accuracy tolerance of less than 1 millimeter. This spatial precision allows the surgical team to plan the shortest, safest trajectory through healthy brain tissue. It minimizes unnecessary exposure and protects critical tracts that govern speech, movement, and vision.
A Paradigm Shift in Neuro-Oncology
We must stop viewing intracranial geography as a static map of independent zip codes. The human brain is a highly interconnected, dynamic organ where the true impact of a lesion depends entirely on its relationship to critical neural networks. Finding where is the most common spot for a brain tumor matters less than decoding how that specific location disrupts the broader neural architecture. Looking at isolated percentages misses the bigger picture. In short: geography is destiny inside the cranium, and our treatment strategies must evolve past simple lesion removal toward preserving network connectivity. Survival metrics will only improve when we treat the brain as an integrated ecosystem rather than a collection of distinct compartments.