The ER tracking monitors are finally quiet, the panic has subsided, but now the real work of staying alive begins. You survive the initial acute event, but the biological landscape inside your chest has fundamentally changed. Many people assume these medications aggressively dissolve the clot like drain cleaner. They do not. Your body handles the cleanup crew duties; the drugs simply freeze the enemy in place. I have seen patients walk out of hospitals feeling entirely cured, completely unaware that the next six months of their lives will be dictated by a tiny, daily pill that carries its own set of terrifying risks.
Understanding the Threat: Why Post-Clot Prescriptions Are Absolutely Non-Negotiable
A pulmonary embolism (PE) is not a static injury; it is a dynamic vascular emergency that leaves a lasting imprint on the coagulation cascade. When a thrombus obstructs the pulmonary bed, the right ventricle of the heart strains against immense pressure, leading to potential right ventricular dysfunction. Data from epidemiological registries indicates that without follow-up pharmacological intervention, the recurrence rate of a venous thromboembolism (VTE) within the first three months approaches a staggering 30 percent. That changes everything because a second event is frequently more catastrophic than the first.
The Delicate Mechanics of the Coagulation Cascade
Where it gets tricky is understanding how our blood switches from a fluid state to a solid plug. The coagulation cascade is a beautiful, hyper-complex domino effect of proteins where Factor Xa and thrombin act as the ultimate gatekeepers. When a PE occurs, this system has gone completely rogue. Anticoagulants do not actually thin the blood's viscosity—contrary to popular belief—but instead disrupt this chemical chain reaction. By throwing a wrench into the enzymatic gears, these medications extend the time it takes for a clot to form, ensuring that the pulmonary vasculature is given a fighting chance to heal through natural fibrinolysis.
Provoked Versus Unprovoked Events: The Diagnostic Turning Point
The duration of your treatment hinges entirely on a single question: why did the clot happen? If you just hopped off an eleven-hour flight from Tokyo to Los Angeles with a swollen calf, or if you underwent a total knee arthroplasty at the Mayo Clinic, your PE is considered "provoked" by a transient risk factor. Standard protocol dictates a fixed three-month treatment window for these scenarios. But what if you were just sitting on your couch, eating breakfast, and suddenly couldn't breathe? Unprovoked embolisms indicate a hidden, systemic vulnerability—perhaps a genetic mutation like Factor V Leiden—and that usually means indefinite, lifelong anticoagulation therapy.
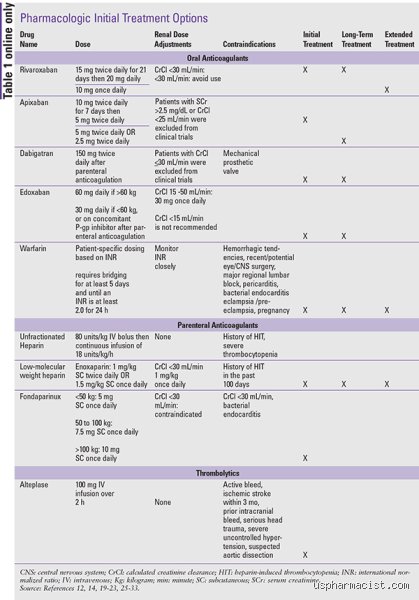
The Acute Phase: The Immediate Lifesavers Deployable in the Hospital Room
The transition from the emergency resuscitation bay to the medical-surgical floor requires an immediate shift in pharmacological strategy. The choice of initial therapy depends on hemodynamic stability; if a patient's blood pressure is crashing, doctors might deploy thrombolytic "clot busters" like alteplase, but for the vast majority, heparinization is the gold standard. This phase is all about speed and precision, utilizing drugs with incredibly short half-lives so that doctors can pivot if internal bleeding complications suddenly arise.
The Classic Standard: Unfractionated Heparin Versus Low-Molecular-Weight Heparin
For decades, clinicians relied exclusively on intravenous unfractionated heparin (UFH), a drug that requires continuous monitoring of the activated partial thromboplastin time (aPTT) every six hours. It is a tedious, needle-poke-heavy process. Enter enoxaparin (Lovenox), a low-molecular-weight heparin (LMWH) administered via subcutaneous injections twice a day based strictly on the patient’s body weight. LMWH offers a far more predictable pharmacokinetic profile, completely eliminating the need for constant laboratory blood draws. Honestly, it's unclear why some institutions still cling to UFH for stable patients, except that UFH can be instantly reversed with protamine sulfate if emergency surgery becomes necessary.
The Threat of Heparin-Induced Thrombocytopenia (HIT)
Yet, there is a dangerous serpent hiding in the heparin grass. A small percentage of patients—roughly 1 to 5 percent exposed to UFH—develop an immune-mediated reaction known as Heparin-Induced Thrombocytopenia. Instead of preventing clots, the patient’s own antibodies activate platelets, causing a paradoxical explosion of new clots throughout the body while dropping the overall platelet count. If HIT is suspected, heparin must be stopped immediately and replaced with an expensive, continuous intravenous infusion of a direct thrombin inhibitor like argatroban or bivalirudin.
The Oral Revolution: Navigating the Era of DOACs and Traditional Warfarin
Once the patient can tolerate oral intake and is heading toward discharge, the conversation shifts to long-term maintenance. For nearly sixty years, the undisputed king of this domain was Vitamin K antagonists. But the pharmaceutical landscape underwent a seismic shift in the 2010s, introducing medications that made recovery vastly more convenient though significantly more expensive.
The Rise of DOACs: Apixaban and Rivaroxaban Take the Crown
Direct Oral Anticoagulants, or DOACs, have fundamentally transformed how we manage pulmonary embolism recovery. Medications like apixaban (Eliquis) and rivaroxaban (Xarelto) directly inhibit Factor Xa without requiring dietary restrictions or routine blood monitoring. Apixaban is typically initiated at a high dose of 10 mg twice daily for the first seven days, followed by a reduction to 5 mg twice daily. Rivaroxaban requires a 15 mg twice-daily loading dose for three weeks, taken strictly with food to ensure proper absorption. People don't think about this enough: missing just one or two doses of a DOAC can leave you dangerously unprotected because these drugs clear the human system much faster than older therapies.
The Old Guard: Why Warfarin Refuses to Entirely Disappear
But what about good old-fashioned warfarin (Coumadin)? It is cheap, it has been used since the 1950s, and it remains the necessary choice for specific patient populations. If you have severe renal failure (a creatinine clearance under 30 mL/min) or suffer from Antiphospholipid Syndrome—an autoimmune clotting disorder—DOACs are notoriously unreliable, making warfarin mandatory. The issue remains that warfarin requires patients to undergo regular International Normalized Ratio (INR) blood tests, aiming for a tight therapeutic target between 2.0 and 3.0. Eat too much spinach or broccoli, and your Vitamin K levels spike, rendering the warfarin completely useless.
Weighing the Options: Head-to-Head Comparisons of Modern Post-PE Regimens
Choosing the right medication after a pulmonary embolism is never a one-size-fits-all clinical decision. It requires balancing the ischemic risk of a recurrent clot against the hemorrhagic risk of a major brain or gastrointestinal bleed. Let us look at how these primary oral agents stack up against one another in real-world clinical practice.
Efficacy and Bleeding Risks: The Large-Scale Trial Data
The landmark AMPLIFY trial, which evaluated apixaban against standard conventional therapy, demonstrated a magnificent 69 percent reduction in major bleeding events, proving that newer does indeed mean safer in many contexts. Similarly, the EINSTEIN-PE study highlighted that rivaroxaban matched the efficacy of older regimens while significantly streamlining the patient experience. As a result: DOACs are now the first-line recommendation by both the American College of Chest Physicians and the European Society of Cardiology. Except that when a major bleed does occur on a DOAC, reversing it requires specific, incredibly high-priced antidotes like andexanet alfa, which are not universally stocked in smaller, rural community hospitals.
The Financial Dilemma and Patient Adherence
The thing is, a drug only works if the patient can actually afford to pick it up from the pharmacy counter. A thirty-day supply of a modern DOAC can easily command over $500 out-of-pocket without premium insurance coverage, whereas a month of warfarin costs less than the price of a fast-food meal. We are far from a perfect system when a patient chooses to split their life-saving pills in half just to make it to their next paycheck. Which explains why a subset of clinicians still aggressively advocate for warfarin; a highly monitored patient on an affordable drug will always fare better than a patient skipping doses of a modern pharmaceutical miracle they simply cannot afford.