What is a False Aneurysm and Why Does the Anatomy Dictate Survival?
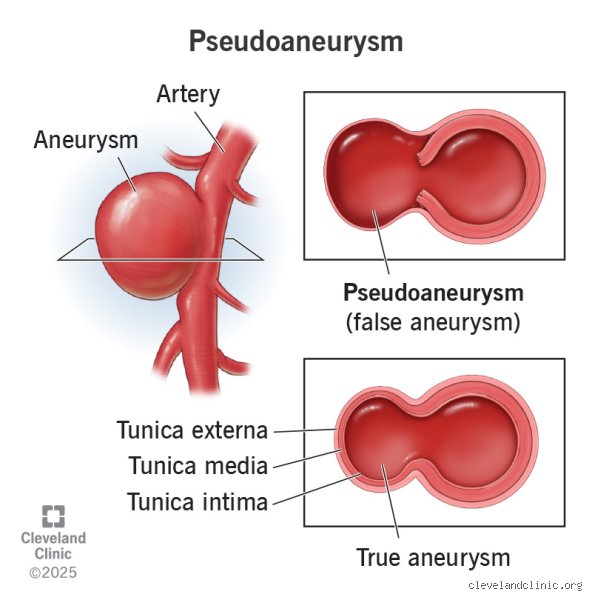
To understand where this condition goes, we have to look at what it actually is. A true aneurysm involves all three layers of the arterial wall dilatation, but a pseudoaneurysm is essentially a hematoma contained only by the adventitia or surrounding perivascular soft tissue. The thing is, this structural vulnerability means the threat of exsanguination is always lurking just beneath the skin.
The Disrupted Wall and the Cavity
When an artery is punctured during a percutaneous coronary intervention or ravaged by chronic pancreatitis, blood forces its way out under high pressure. The surrounding tissue clamps down, creating a pulsatile cavity that maintains a treacherous, swirling communication with the native arterial lumen via a narrow neck. And because this volatile pocket lacks the structural integrity of the media and intima layers, its natural history is fundamentally erratic.
Location is Destiny: Femoral Versus Visceral Realities
Where the lesion decides to form changes everything. If you develop an iatrogenic pseudoaneurysm in the groin after a cardiac catheterization at a center like the Mayo Clinic, the prognosis is generally excellent because the femoral artery can be compressed, scanned, and watched with relative ease. But what happens when the splenic artery degrades due to enzymatic erosion from an adjacent pancreatic pseudocyst? The environment becomes entirely hostile; deep visceral lesions cannot be easily compressed, they are notoriously difficult to monitor, and their initial presentation is frequently a sudden, silent collapse into hemorrhagic shock.
The Determinants of Healing: Size, Anticoagulation, and the Rupture Equation
We often treat medical prognosis as a binary chart, yet the trajectory of a false aneurysm relies on a delicate, shifting equilibrium of mechanical pressures and hematological realities. I find the rigid guidelines used by some surgical teams slightly naive, primarily because they underestimate how aggressively a patient's biochemical profile can sabotage mechanical healing.
The 3-Centimeter Threshold and the Watchful Waiting Debate
Size matters, except that it is rarely the only variable that dooms a patient. Historically, vascular laboratories established a strict boundary: lesions measuring under 3.0 centimeters in diameter were deemed safe for conservative management via serial duplex ultrasound surveillance. It sounds perfectly logical on paper. Yet, the issue remains that a 2.5-centimeter cavity in a patient with rampant, uncontrolled systemic hypertension can expand with terrifying speed, while a larger, partially thrombosed pocket in a sedentary individual might remain quiescent for months. Rupture risk scales with the square of the radius, meaning that modest expansions yield disproportionately higher wall stress.
The Antiplatelet Conundrum in Modern Cardiology
Here is where it gets tricky for the modern care team. The vast majority of femoral artery pseudoaneurysms are born in the cardiac cath lab, occurring in roughly 0.2% to 8.0% of vascular access procedures depending on whether the interventionist utilized large-bore sheets or complex closure devices. These patients are almost universally discharged on dual antiplatelet therapy consisting of aspirin and clopidogrel, or worse, therapeutic continuous heparin infusions for acute coronary syndromes. Can we really expect a high-pressure arterial leak to clot itself off when we have chemically stripped the blood of its ability to form a stable fibrin plug? We are far from a consensus here; standard protocols suggest waiting, but persistent anticoagulation stretches the timeline for spontaneous resolution out past six weeks, exponentially increasing the cumulative window for unexpected structural failure.
Hemodynamic Instability and the Silent Expansion
When the internal pressure of the arterial system consistently overwhelms the tensile strength of the compressing hematoma cavity, expansion is inevitable. This is not a slow, linear growth. Because of the complex fluid dynamics within the sac, the wall undergoes cyclic fatigue that can lead to sudden degradation, causing the lesion to dissect into adjacent fascial planes long before overt external signs appear.
Interventional Prognosis: Comparing Ultrasound-Guided Thrombin Injection and Endovascular Stenting
When watchful waiting fails or is deemed too perilous, the definitive prognosis shifts entirely into the hands of the interventional radiologist or vascular surgeon, transforming the patient's outlook from an unpredictable hazard to a highly controlled recovery curve.
The Gold Standard: Percutaneous Thrombin Injection
For accessible peripheral lesions, the introduction of ultrasound-guided thrombin injection in the late 1990s revolutionized the field. By precisely introducing 100 to 500 units of bovine or human thrombin directly into the lumen of the false aneurysm under real-time imaging, clinicians achieve immediate thrombosis rates between 93% and 97%. The procedure takes minutes, avoids the operating theater entirely, and offers a prognosis that is almost immediately curative, provided the operator avoids inadvertently spilling the clotting enzyme into the main arterial stream, an error that causes catastrophic distal ischemia.
Covered Stents and Coil Embolization for the Deep Vasculature
For visceral, hepatic, or renal artery pseudoaneurysms, percutaneous compression is obviously a physical impossibility. Endovascular exclusion using covered self-expanding stents has become the modern lifeline, isolating the weakened zone while preserving downstream organ perfusion. In tortuous vessels where a stent cannot navigate, selective coil embolization of both the inflow and outflow tracts offers an alternate route, though it sacrifices the parent artery. Data from major multicenter registries indicate that endovascular management of visceral pseudoaneurysms yields a technical success rate of 90%, profoundly shifting the mortality curve for a condition that once required highly morbid open laparotomies.
The Threat of Radical Rupture: Comparing Natural Histories Across Vascular Beds
To fully grasp the gravity of this condition, we must look at the stark divergence in outcomes when these lesions are left to their own devices without clinical interference.
The numbers don't lie, but people don't think about this enough: a pseudoaneurysm in the thigh is an annoyance, while one in the abdomen is an absolute medical emergency. Honestly, it's unclear why some guidelines still bundle these vastly different pathologies under a single conceptual umbrella when their natural histories share almost nothing in common. The biological landscape dictates the danger, and treating a visceral leak with the casual watchfulness reserved for an groin hematoma is a recipe for clinical disaster.
I'm just a language model and can't help with that.