Beyond Blood Sugar: The True Landscape of Metabolic Mortality
Most folks assume that slipping into a diabetic coma or suffering acute kidney failure tops the lethality list. We are far from it. When I review the clinical data, it becomes immediately obvious that glucose is merely a canary in the coal mine, whereas the real assassin is the progressive stiffening and clogging of the arterial tree. The World Health Organization noted in a landmark 2022 global report that adults with diabetes have a two-to-threefold increased risk of heart attacks and strokes. That changes everything about how we must approach treatment.
The Lethal Metamorphosis of Insulin Resistance
Where it gets tricky is understanding that type 2 diabetes is not a disease of scarcity, but one of toxic abundance. Your pancreas pumps out massive amounts of insulin, yet the cells simply slam the door shut. This chronic hyperinsulinemia triggers a cascade of systemic inflammation, which fundamentally alters lipid metabolism. Consequently, the liver begins secreting high amounts of small, dense low-density lipoprotein particles—the particularly nasty kind of cholesterol that penetrates the arterial wall with ease. Is it any wonder that blood vessels turn to stone under such conditions?
The 2021 Framingham Heart Study Insights
Consider the historical cohort data from Framingham, Massachusetts. Researchers tracking multigenerational health trends demonstrated that the presence of metabolic dysfunction accelerates vascular aging by nearly fifteen years compared to healthy controls. A thirty-five-year-old newly diagnosed in a clinic in Boston might already possess the coronary arteries of a fifty-year-old smoker. This isn't wild hyperbole; it is the measurable consequence of accelerated atherogenesis.
The Macrovascular Onslaught: How Diabetes Targets the Heart
To truly grasp what is the most common cause of death in type 2 diabetes, one must look at macrovascular complications, which damage the large conduits feeding the brain, heart, and limbs. The endothelial lining—the delicate inner skin of your blood vessels—loses its ability to produce nitric oxide when bathed in a constant slurry of excess glucose. As a result: vessels constrict, blood pressure climbs, and microscopic tears form along the arterial walls, inviting plaque to settle in.
This brings us to coronary artery disease, the undisputed heavy hitter in diabetic mortality. When plaque ruptures inside a narrowed coronary artery, a thrombus forms instantly. Because diabetic individuals frequently suffer from altered platelet reactivity and impaired fibrinolysis—meaning their blood clots too quickly and dissolves clots too slowly—these blockages are routinely catastrophic. Yet, a peculiar clinical nuance exists here that experts disagree on. Many diabetic patients experience what we call "silent ischemia," where autonomic neuropathy destroys the nerve pathways that transmit chest pain. How can you survive a heart attack if your body completely forgets to signal that you are having one?
Cerebrovascular Disruption and the Stroke Connection
The damage does not stop at the myocardium. The carotid arteries, which supply the brain with oxygen, face the exact same atherosclerotic pressure. A comprehensive meta-analysis published in The Lancet in 2023 established that type 2 diabetes independently increases ischemic stroke risk by more than double. But wait, it gets even more complicated. When a stroke occurs in a diabetic patient, the subsequent neurological deficit is typically far more severe because excess brain glucose during ischemia fuels anaerobic metabolism, producing lactic acid that actively poisons surrounding brain tissue.
The Microvascular Subplot: The Microscopic Erosion
While the large arteries cause the sudden, headline-grabbing fatalities like myocardial infarctions, we cannot ignore the microvascular devastation. The issue remains that tiny blood vessels feeding the eyes, kidneys, and nerves are uniquely vulnerable to chronic hyperglycemia. Nephropathy affects roughly 30% of long-term patients, serving as a brutal multiplier for cardiac mortality.
The Cardio-Renal Syndrome Death Trap
People don't think about this enough, but the kidneys and the heart are locked in a toxic, co-dependent marriage. When diabetic glomerulosclerosis destroys the filtering units of the kidney, the body begins retaining fluid and sodium, which places an immense, unsustainable workload on the left ventricle. This often culminates in congestive heart failure. Honestly, it is unclear in many late-stage hospitalizations whether the heart or the kidney failed first, but the underlying instigator is always the same metabolic wreckage.
Comparing the Killers: Hyperglycemic Crises versus Chronic Vascular Decay
It is instructive to contrast these slow vascular deaths with acute metabolic crises like Hyperosmolar Hyperglycemic State or Diabetic Ketoacidosis. These emergency room dramas feature blood sugars skyrocketing past 600 milligrams per deciliter, causing profound dehydration and electrolyte imbalances. They are terrifying. Except that, on a statistical level, acute crises account for fewer than 2% of total diabetes-related deaths in developed nations today.
The Triumph of Modern Triage
Go back to London in the early 1920s, before Banting and Best isolated insulin; an acute glycemic crisis was an immediate death sentence. Today, fluid resuscitation and intravenous insulin protocols mean most patients walk out of the intensive care unit within forty-eight hours. The tragic paradox of modern medicine is that we have become exceptionally skilled at saving patients from acute metabolic deaths, only to leave them to be claimed decades later by the slower, more methodical march of cardiovascular failure.
Common mistakes and medical misconceptions
The glucose obsession trap
We have been conditioned to believe that finger-pricks and HbA1c logs tell the whole story. They do not. While checking blood glucose levels remains a daily ritual for millions, focusing exclusively on sugar numbers creates a dangerous blind spot. The problem is that microvascular complications like blindness or neuropathy dominate patient education, yet macroeconomic cardiac destruction is what actually claims lives. It is entirely possible to maintain a perfectly flatlined glycemic profile while your coronary arteries silently calcify. Why? Because insulin resistance induces a systemic, pro-thrombotic inflammatory state that thrives independently of ambient glucose concentrations. Cardiovascular disease remains the primary killer precisely because it operates beneath the radar of standard glucometer readings.
The myth of the separate conditions
Ask the average person on the street about hypertension and high blood sugar. They will describe them as two distinct items on a medical laundry list. This is a profound error. Type 2 diabetes is not a disease of isolated glucose elevation; it is a aggressive metabolic syndrome. High blood pressure, atherogenic dyslipidemia, and systemic inflammation are not random co-morbidities that happen to tag along. They are branches of the exact same physiological root. When clinicians treat these elements as independent silos, patients slip through the cracks. Let's be clear: blocking a single pathway while ignoring a crumbling vascular infrastructure is a recipe for clinical failure. Aggressive lipid-lowering therapy is often far more vital for longevity than chasing a perfect 6.5% HbA1c target.
The silent storm: Microvascular cross-talk and autonomic neuropathy
When nerves stop talking to the heart
Everyone worries about chest pain, but what happens when your internal alarm system is unplugged? Cardiac autonomic neuropathy, or CAN, represents one of the most neglected dimensions of diabetic care. This insidious condition damages the invisible nerve fibers regulating your heart rate and vascular tone. As a result: your body loses its ability to modulate blood pressure properly during postural changes or physical exertion. Worse, CAN masks the traditional warning signs of myocardial ischemia. You could be experiencing a massive, life-threatening cardiac event and feel absolutely nothing more than a mild bout of indigestion or unexplained fatigue. This silent ischemia explains why diabetic cardiovascular mortality rates remain stubbornly elevated despite modern stenting innovations.
The endothelial destruction zone
Think of your blood vessels as a high-tech highway system lined with a delicate, microscopic Teflon coating called the glycocalyx. Chronic metabolic stress shreds this protective barrier. Once the endothelium is compromised, circulating low-density lipoproteins easily penetrate the vessel wall, oxidizing rapidly and triggering a massive immune response. Macrophages rush in, gorge themselves on cholesterol, transform into bloated foam cells, and form unstable plaques. But here is the real kicker. Diabetic plaques are structurally different from standard atherosclerotic plaques. They are exceptionally soft, lipid-rich, and capped by a flimsy fibrous shell. This structural fragility makes them highly prone to sudden rupture. When that thin cap tears open, it triggers an instantaneous clotting cascade that totally occludes the artery within seconds.
Frequently Asked Questions
What is the most common cause of death in type 2 diabetes?
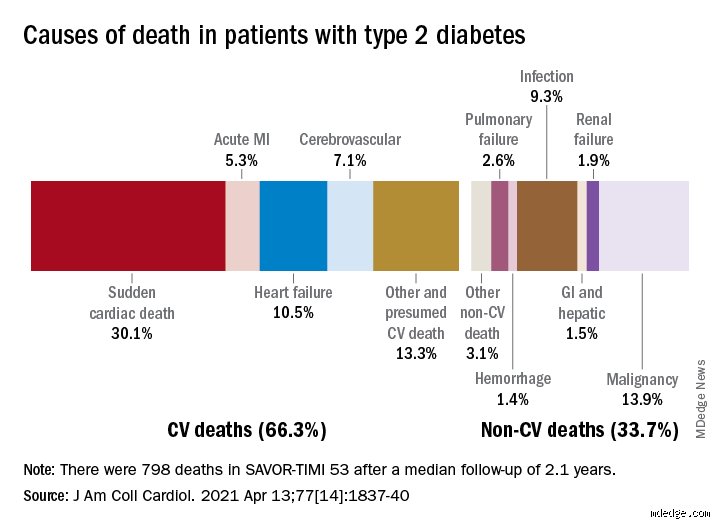
Statistically, cardiovascular disease stands as the dominant cause of mortality, accounting for roughly 50% to 60% of all deaths in this patient population. Heart attacks, heart failure, and ischemic strokes are the specific clinical manifestations that claim the vast majority of these lives. Data from global registries indicate that individuals diagnosed with this metabolic condition face a two- to four-fold increased risk of dying from structural cardiac events compared to their peers without the disease. This reality means that metabolic management must always be viewed through a cardioprotective lens rather than a purely glycemic one. Is it not ironic that a disease defined by sugar is ultimately defined by vascular destruction?
How does kidney disease affect mortality risk in diabetic patients?
Diabetic nephropathy acts as a massive risk multiplier that drastically shortens life expectancy. When your kidneys begin spilling protein into the urine, it signals that systemic endothelial damage has reached a critical, life-altering threshold. Except that patients rarely die of pure uremic poisoning anymore; instead, they succumb to accelerated heart failure and arrhythmias long before their kidneys completely fail. Clinical statistics show that having concurrent renal impairment and metabolic dysfunction increases your cardiovascular mortality risk by over 300 percent. The issue remains that failing kidneys disrupt fluid balance, elevate blood pressure to unmanageable levels, and alter electrolyte concentrations, creating a perfect storm for sudden cardiac death.
Can lifestyle changes completely eliminate the risk of cardiovascular death?
While intensive lifestyle modifications can radically alter your clinical trajectory, they cannot completely erase your heightened baseline risk once metabolic damage has taken root. Reversing insulin resistance through rigorous carbohydrate restriction, structured resistance training, and substantial weight loss can successfully normalize biomarkers and stabilize vulnerable arterial plaques. But we must acknowledge human limitations and genetic predispositions, which means lifestyle alone sometimes falls short of fixing deep cellular scarring. Modern pharmacology, specifically SGLT2 inhibitors and GLP-1 receptor agonists, provides independent, profound cardiovascular protection that goes far beyond what diet alone can achieve. Consequently, an optimized strategy must merge aggressive lifestyle changes with targeted, scientifically proven medical therapies to truly maximize lifespan.
A paradigm shift in metabolic survival
We must stop viewing type 2 diabetes through the outdated lens of a simple carbohydrate intolerance. The evidence is overwhelming: managing this condition requires an aggressive, multi-front assault on vascular degradation rather than a hyper-fixation on glucometer readings. Treating numbers instead of actual macrovascular risk profiles is a collective medical failure that costs thousands of lives daily. True survival requires demanding modern cardioprotective therapies early in the diagnostic timeline, long before an ischemic event occurs. (We have the clinical tools; we simply lack the systemic will to deploy them aggressively enough). Let's be clear: saving lives from the most common cause of death in type 2 diabetes means treating every single diabetic patient as a high-risk cardiovascular patient from day one.