Walk into any psychiatric unit or community clinic, and you will hear clinicians tossing around the term "formulation" like confetti. We love it because a diagnosis—say, Major Depressive Disorder, code 296.22—tells you almost nothing about the human being sitting across from you. It is a label, a shorthand file folder. The real clinical heavy lifting happens when we ask why this specific person developed this particular storm at this exact moment in their life. That is where the 4 Ps framework comes in, acting as the scaffold for the Case Formulation approach popularized by behavioral pioneers in the late 20th century. I used to think the model was overly simplistic, a mere teaching tool for interns, but years of unpacking complex trauma taught me that without this specific structural anchor, clinical assessments easily degenerate into guesswork. It is about organizing chaos.
The Historical Shift Toward Dynamic Formulations in Clinical Practice
Psychiatry spent decades obsessed with classification. When the American Psychiatric Association published the DSM-III in 1980, it shifted the entire field toward a strict, neo-Kraeplinian biomedical model focused heavily on reliability and symptom checklists. But treating mental health like a purely dermatological rash—see a spot, name the spot—left a massive intellectual void. Practitioners realized that two patients with the exact same diagnosis often required completely opposite treatment paths. Which explains why George Engel’s Biopsychosocial Model gained such rapid traction during this era, forcing clinicians to look at the intersection of biology and social environments.
Why Symptoms Alone Never Tell the Whole Story
Imagine treating a patient, let's call him David, who presented to a Boston outpatient clinic in October 2022 with severe panic attacks. A purely diagnostic assessment sees the racing heart, the avoidance behavior, and labels it Panic Disorder. Simple, right? Except that the label completely misses the fact that David's father died of a sudden myocardial infarction at the exact same age David is now. The symptom is merely the tip of an iceberg that drifts deep into historical waters. Where it gets tricky is realizing that a symptom is often an adaptation, a distorted way of coping with an underlying vulnerability that the patient cannot yet articulate.
The Case Formulation vs. The Diagnostic Checklist
Let’s be honest, it's unclear why some clinics still rely solely on tick-boxes when the evidence for formulation is so overwhelming. A diagnostic checklist is static; it captures a frozen snapshot of misery. Case formulation, using the 4 Ps matrix, functions more like a cinematic narrative that tracks movement, causality, and resistance over time. The issue remains that insurance companies demand the static code, while effective psychotherapy demands the fluid story.
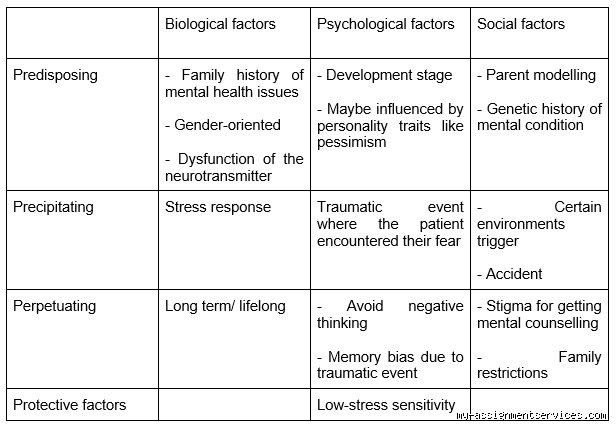
Deconstructing the Matrix: Predisposing and Precipitating Factors
To understand the timeline of suffering, we have to split the past from the present. The first two Ps deal with the fuel and the match. Predisposing factors are the silent vulnerabilities built into a person's biology or early life, long before any clinical symptoms actually manifest. Think of these as the structural weaknesses in a house. Then come the precipitating factors, which are the immediate stressors or life events that breach those weaknesses and spark the acute crisis. It is the classic stress-diathesis model in action, where nature and nurture finally collide.
Predisposing Factors: The Latent Vulnerabilities
What makes a person fragile in the first place? Genetic load, such as a family history of bipolar affective disorder, sets a baseline biological vulnerability. But we cannot ignore early childhood experiences like chronic emotional neglect or early parental loss. A landmark 1998 study on Adverse Childhood Experiences (ACEs) proved that early trauma fundamentally rewires the hypothalamic-pituitary-adrenal axis, permanently altering how a person handles stress in adulthood. These factors don't cause depression directly, yet they prime the psychological canvas, creating silent cognitive schemas—like "I am inherently unlovable"—that sit quietly for decades waiting to be activated.
Precipitating Factors: The Acute Triggers
This is the catalyst, the match dropped onto dry brush. A precipitating factor is an identifiable event that occurred shortly before the onset of symptoms, such as a sudden job loss, a divorce, or even a physical illness. Take a patient who experiences a severe bout of insomnia after a car accident in downtown Chicago. The accident is the precipitant. People don't think about this enough: sometimes the precipitant seems minor to an outsider, but because it links directly to an old, hidden predisposing vulnerability, that changes everything. It acts like a key turning in a lock that has been rusted shut for years.
The Maintenance Mechanisms: Perpetuating Factors in Mental Distress
Why doesn't the wound heal on its own? This is where we look at perpetuating factors, the third P, which are the variables that keep the condition going once it has started. These are the feedback loops, the behavioral traps, and the environmental reinforcers that actively prevent recovery. If you don't identify and break these mechanisms, any therapeutic intervention you try will simply slide off the surface without changing the system.
Behavioral Avoidance and Cognitive Distortions
When a person is anxious, they avoid the things that scare them. It makes perfect sense in the short term because avoidance drops their anxiety levels down to zero immediately. But that temporary relief is exactly what perpetuates the disorder over time, because the individual never learns that their feared catastrophe won't actually happen. In cognitive behavioral therapy, we call this the maintenance cycle of anxiety. In short: the safety behavior becomes the actual disease. Add to this rumination cycles and negative automatic thoughts, and the patient effectively traps themselves inside an internal echo chamber of despair.
Systemic and Environmental Reinforcers
Sometimes the problem isn't just inside the patient's head; it is embedded in their living room. Interpersonal dynamics can heavily perpetuate psychological distress. A well-meaning partner who constantly steps in to manage a patient’s agoraphobia might actually be reinforcing the dependency, a concept known in family systems theory as systemic accommodation. Furthermore, ongoing systemic stressors like chronic financial strain, living in an unsafe neighborhood, or facing systemic discrimination act as constant, unyielding heavy weights that keep the individual submerged in chronic stress, making recovery nearly impossible without structural changes.
Flipping the Script: The Vital Role of Protective Factors
Clinical psychology has historically been a bit cynical, focused almost entirely on what is broken, deficient, or traumatized. The fourth P, protective factors, radically corrects this bias by mapping out the patient's strengths, assets, and resilience mechanisms. This is not about superficial, toxic positivity; it is a cold, calculated inventory of the internal and external resources the patient can deploy to fight back against their illness. Honestly, it's where the actual hope in a treatment plan lives.
Internal Resilience and Coping Assets
Some people possess an innate psychological elasticity. Internal protective factors include a high level of emotional intelligence, solid problem-solving skills, and a history of successful coping in past crises. A strong therapeutic alliance relies on these; we need to know what worked for the patient when they faced adversity five years ago. Even a baseline level of psychological insight or a quirky, dark sense of humor can serve as a massive shield against the corrosive effects of a severe depressive episode. Do they have a hobby that grounds them? Can they still find meaning in their work? These are the foundations upon which we build behavioral activation plans.
External Support Systems and Social Capital
Isolation is a killer in mental health. Therefore, the presence of a supportive, non-judgmental social network is often the single greatest predictor of positive clinical outcomes. This could be a devoted spouse, a tight-knit religious community in rural Ohio, or even a reliable peer-support group. Having just one person who truly validates their experience can completely change the trajectory of a major crisis. As a result: an assessment that fails to document these external assets is incomplete, leaving the clinician blind to the very resources that could prevent an emergency psychiatric hospitalization during a severe relapse.