The Clinical Reality: Deconstructing Acute Pancreatitis as a True Medical Emergency
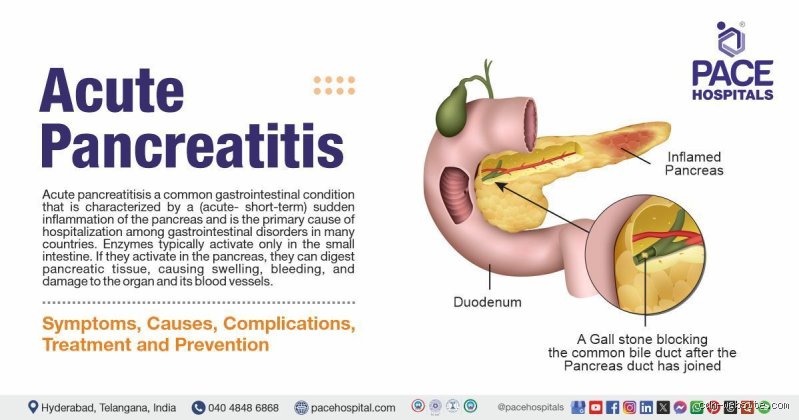
To truly understand why this condition triggers such alarm bells in hospitals from London to Tokyo, we have to look at the anatomy of disaster. The pancreas is a dual-purpose powerhouse, producing both digestive enzymes and insulin. Normally, these enzymes travel safely to the small intestine before waking up. In acute pancreatitis, something disrupts this pipeline—often a rogue gallstone blocking the bile duct or a sudden spike in blood triglycerides—and the enzymes activate prematurely while still trapped inside the pancreatic tissue. Imagine a bottle of industrial acid leaking inside your abdomen; that changes everything. The resulting localized destruction is only the first domino to fall. What starts as cellular death within a single organ can rapidly trigger a systemic inflammatory response syndrome (SIRS), which cascades throughout the entire human body. Is it any wonder that clinicians treat severe cases with the same urgency as a major stroke or a massive myocardial infarction? Because the pancreas sits in such close proximity to major abdominal blood vessels, the localized necrosis can lead to massive internal hemorrhaging, a complication that requires immediate surgical or radiological intervention to prevent exsanguination.
The Spectral Shift from Mild Discomfort to the Intensive Care Unit
Medical students are often taught the Ranson criteria or the APACHE II scoring system to predict just how badly a patient's case will go sideways. Yet, predicting the trajectory remains notoriously difficult during the first 24 hours of admission. Mild acute pancreatitis usually involves a short hospital stay, a few days of intravenous fluids, and some bowel rest. But when the disease crosses the threshold into the severe category, we are talking about extensive pancreatic necrosis where portions of the organ literally die. This necrotic tissue is a ticking time bomb; if it becomes infected by gut bacteria, the mortality rate skyrockets toward 40% to 50% without aggressive intervention.
Why General Practitioners Fear the Delayed Diagnosis
I once watched an emergency room physician mistake early-stage pancreatic inflammation for a standard case of gastritis, a mistake that nearly cost the patient their life when their kidneys began shutting down twelve hours later. People don't think about this enough: the pain of acute pancreatitis is often described as a boring, drilling sensation that radiates straight through to the back, forcing patients into a fetal position. It is not something you can easily ignore with an antacid. When a patient presents with this classic posture, a rapid serum amylase or lipase test showing levels at least three times the upper limit of normal is required to confirm what the body already knows.
Navigating the Insurance Maze: When Does Inflammation Count as a Critical Illness?
Where it gets tricky is translating this physiological chaos into the cold, bureaucratic language of financial indemnity. If you flip through a standard critical illness insurance policy document, you will rarely find "acute pancreatitis" listed as a standalone covered condition in the same way you see cancer or stroke. Instead, policyholders must usually qualify under broader, more terrifying umbrella terms like major organ failure or chronic, irreversible pancreatic dysfunction. But why should a patient fighting for their breath on a ventilator have to argue over semicolons in a insurance contract? The issue remains that insurance companies differentiate sharply between a transient, acute event that resolves without permanent damage and a catastrophic illness that permanently alters your earning capacity. To trigger a payout, most policies require evidence that the acute event caused persistent, measurable impairment—such as requiring ongoing dialysis due to secondary acute kidney injury, or permanent mechanical ventilation for acute respiratory distress syndrome (ARDS).
The Fine Print of Severe Acute Pancreatitis Claims
Let us look at a concrete example: a policy issued by a major provider in 2024 might stipulate that a digestive system disease only qualifies for a lump-sum payout if it results in total and permanent inability to perform at least three activities of daily living, or if it necessitates a total pancreatectomy. That means if you survive a harrowing three-week stint in the ICU with severe necrotizing pancreatitis but manage to walk out of the hospital with your pancreas partially intact, your claim might still be denied. It is a harsh, binary system that ignores the grueling, months-long recovery period that survivors face as they deal with profound muscle wasting and chronic fatigue.
The Debate Among Underwriters Regarding Chronic Progression
Honestly, it's unclear why the insurance industry remains so hesitant to modernize its definitions regarding pancreatic diseases. Some underwriting experts argue that because a single episode of acute pancreatitis can completely resolve, listing it outright would lead to a flood of claims for mild cases that required nothing more than a 48-hour observation stay. Yet, data shows that roughly 20% of patients who experience an acute attack will go on to suffer recurrent episodes, and a significant portion of those will ultimately develop chronic pancreatitis, a debilitating condition characterized by permanent tissue scarring, intractable pain, and exocrine pancreatic insufficiency.
The Biological Cascade: What Happens When the Pancreas Self-Destructs?
To comprehend why this illness occupies such a dreaded status in critical care medicine, we must examine the cellular warfare occurring within the retroperitoneal space. When trypsinogen is prematurely converted to active trypsin within the pancreatic acinar cells, it sets off a chain reaction that activates other destructive enzymes like elastase and phospholipase A2. Elastase dissolves the elastic fibers of blood vessels, causing widespread capillary leaking and profound fluid shifts. This is not a localized problem. As litres of fluid escape from the circulatory system into the interstitial spaces of the abdomen—a phenomenon known as third-spacing—the patient's blood pressure plummets, plunging them into hypovolemic shock. This profound drop in perfusion is the direct catalyst for multi-organ dysfunction syndrome (MODS), as the kidneys, lungs, and heart are deprived of oxygenated blood.
The Role of Gallstones and Alcohol in Triggering Mitochondrial Failure
In Western societies, gallstones and heavy alcohol consumption account for approximately 75% of all acute pancreatitis cases. While a gallstone physically impacts the ampulla of Vater, alcohol acts as a direct cellular toxin, altering cell membrane fluidity and disrupting calcium signaling within the acinar cells. This massive influx of intracellular calcium overloads the mitochondria, halting ATP production and forcing the cell into a state of necrotic ruin. This cellular death releases damage-associated molecular patterns (DAMPs) into the bloodstream, alerting the immune system and triggering a massive, uncoordinated release of pro-inflammatory cytokines like TNF-alpha and interleukin-1.
Comparing Pancreatic Crisis to Other Critical Systemic Failures
When we place acute pancreatitis alongside other universally recognized critical illnesses, the comparisons are eye-opening. Consider acute myocardial infarction; a coronary artery is blocked, heart muscle dies, and the threat is immediate but largely localized to cardiovascular hemodynamics. In contrast, severe acute pancreatitis mimics the systemic devastation of advanced sepsis or third-degree burns covering a large percentage of the body. The sheer volume of fluid resuscitation required in the first 24 hours of a pancreatic crisis—often between 250 to 500 milliliters per hour of isotonic crystalloid solution—is practically unique to this condition, requiring meticulous central venous pressure monitoring to avoid flooding the patient's lungs.
Acute Pancreatitis Versus Acute Appendicitis: A Dangerous Confusion
Except that people sometimes confuse the two because they both end in the suffix that denotes inflammation. We are far from a simple appendix removal here; an appendectomy is a straightforward, routine surgical procedure with a mortality rate near zero. You cannot simply cut out a inflamed, hemorrhagic pancreas during the acute phase of the illness without causing catastrophic, fatal bleeding. Modern medical consensus dictates a hands-off approach to the pancreas during the initial weeks of an attack, relying instead on supportive care and delayed, minimally invasive step-up interventions only if infected necrosis is confirmed by radiologists.