The Ghost in Your Abdomen: What Actually Happens When the Pancreas Self-Destructs
People don't think about this enough: the pancreas is essentially a biological hand grenade. It sits quietly behind your stomach, manufacturing enzymes so incredibly volatile that they can dissolve a steak in minutes. In a healthy body, these enzymes—trypsin, chymotrypsin, lipase—remain dormant until they travel safely into the duodenum. But when inflammation strikes, everything goes sideways. The enzymes activate prematurely inside the pancreatic parenchyma itself. It is a terrifying process called autodigestion.
The Slippery Slope from Acute Edema to Chronic Necrosis
You might think an attack is just a one-off fluke. I used to believe that mild acute episodes were completely reversible, but the emerging clinical data tells a far more sinister story. Every single bout of acute inflammation leaves behind micro-scarring. Fibrogenesis starts almost immediately, triggered by the activation of pancreatic stellate cells, which lay down collagen like a runaway construction crew. Think of it like a localized burn that forms thick, restrictive scar tissue inside the organ. If this happens repeatedly, the organ loses its compliance, its blood supply strangles, and you slide down the path toward chronic pancreatitis.
The Anatomy of Pain: Why It Feels Like an Iron Fist
Why does the pain radiate directly to your back? Because the pancreas is a retroperitoneal organ, tightly packed against the celiac plexus nerve bundle. When the tissue swells, it compresses these nerves mercilessly. It is an agonizing, boring sensation that worsens after eating even a single grape. Honestly, it's unclear why some people experience mild discomfort while others require high-dose intravenous fentanyl in the intensive care unit. This unpredictability is exactly where it gets tricky for clinicians trying to map out a long-term management strategy.
Immediate Biochemical Interventions to Halt Structural Destruction
The thing is, you cannot simply wish the inflammation away once the cascade begins. You need to manipulate your systemic biochemistry to give the tissue a chance to cool down. In the famous 2012 Atlanta Classification system for acute pancreatitis, fluid resuscitation was identified as the absolute linchpin of early management, yet we are still arguing about the specific mechanics of how to do it right.
Aggressive Hydration: The Ringers Lactate Conundrum
For decades, emergency rooms pumped patients full of standard normal saline. That changes everything when you look at recent clinical trials from the University of Pittsburgh Medical Center. Researchers found that Lactated Ringers solution reduces systemic inflammatory response syndrome (SIRS) significantly faster than saline. Why? Because normal saline can induce a hyperchloremic metabolic acidosis, which actually exacerbates the activation of zymogens within the acinar cells. We want to keep the serum pH slightly alkaline to discourage trypsinogen from morphing into its destructive active form. But you have to balance this carefully—over-hydrating a patient can lead to acute respiratory distress syndrome (ARDS) or abdominal compartment syndrome.
Pancreatic Rest and the Fallacy of Starvation
We used to put patients on strict "NPO" (nothing by mouth) status for weeks, forcing them to rely on total parenteral nutrition through a central line. That was a mistake. Modern gastroenterology has pivoted sharply toward early enteral nutrition within 24 to 48 hours of admission. If you keep the gut completely empty, the intestinal mucosal barrier breaks down. Bacteria from your colon then translocate across the gut wall, migrate through the portal vein, and infect the necrotic pancreatic tissue. That turns a sterile inflammation into an infected necrosis, which carries a staggering mortality rate of up to 30 percent.
Lifestyle Architectures: How to Stop Pancreatitis from Getting Worse Through Daily Habits
If you have survived the initial hospitalization, your primary goal is preventing the next strike. This requires a ruthless overhaul of your metabolic inputs. The pancreas is incredibly unforgiving; it remembers every single insult you throw at it.
The Total Cessation of Ethanol and Nicotine
Let us be completely blunt here. If you continue to drink alcohol after a diagnosis of alcohol-induced pancreatitis, you are actively destroying your life. There is no safe limit—we are far from it. Ethanol is metabolized by the pancreas into toxic metabolites like fatty acid ethyl esters, which destabilize lysosomal membranes within the acinar cells. But here is the piece of advice that surprises most people: you must stop smoking immediately too. Cigarette smoke acts synergistically with alcohol. Nicotine alters calcineurin signaling, accelerating the progression from acute to chronic disease at an alarming rate. It is a dual threat that most patients ignore because they focus entirely on the bottle.
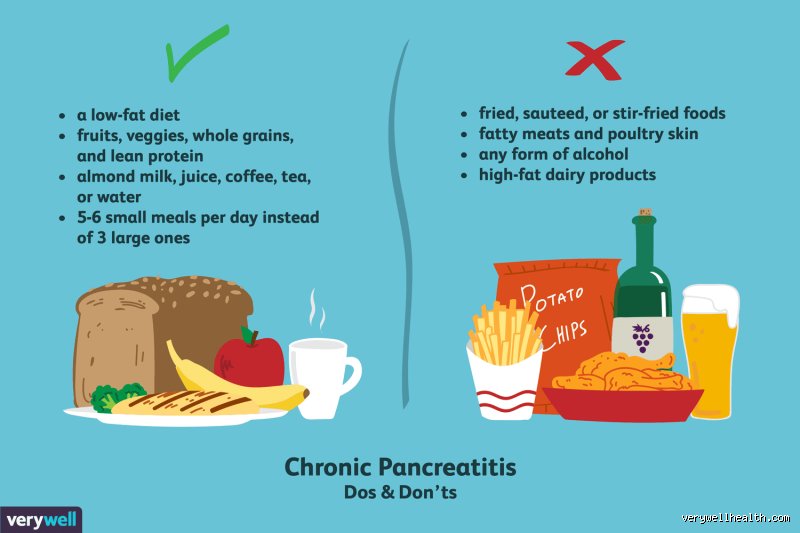
The Radically Modified Low-Fat Diet Protocol
Every time you ingest fat, your duodenum secretes a hormone called cholecystokinin (CCK). This hormone signals your pancreas to pump out digestive enzymes. If the organ is inflamed, that hormonal signal is like whipping a exhausted horse. Your daily fat intake should ideally stay below 20 to 30 grams total, distributed evenly across five or six tiny meals. Focus on medium-chain triglycerides (MCTs), which can be absorbed directly by the enterocytes without requiring pancreatic lipase for breakdown. A typical breakfast might look like egg whites cooked in a dry pan with a slice of dry sourdough toast—bland, uninspiring, but safe.
Comparing Therapeutic Pathways: Enzyme Replacement vs. Surgical Denervation
When conservative measures fail to control the chronic pain and malabsorption, you face a fork in the road. You must choose between biochemical supplementation and invasive structural alteration.
Pancreatic Enzyme Replacement Therapy (PERT)
When the pancreas has lost more than 90 percent of its exocrine capacity, you develop steatorrhea—foul, floating, fatty stools. This is where PERT becomes mandatory. Brands like Creon or Zenpep deliver porcine-derived lipases and proteases directly into your digestive tract. The trick is timing: you must take these capsules with the very first bite of your meal, not halfway through, and certainly not at the end. They mimic the natural physiology of digestion, taking the workload off your scarred organ. Yet, the cost can be prohibitive, often running into hundreds of dollars per month without top-tier health insurance.
Surgical Options and the Frey Procedure
What happens when the main pancreatic duct becomes so tortuous and blocked with calcium stones that the pressure inside the organ skyrockets? Medicine can no longer bridge the gap. Surgeons at the Mayo Clinic frequently utilize the Frey procedure, which combines a local resection of the diseased pancreatic head with a lateral pancreaticojejunostomy. They essentially fillet the duct open and sew it directly to the small intestine to relieve the backpressure. It is an intense, irreversible surgery. It works beautifully for pain relief in about 75 percent of carefully selected patients, but it does nothing to restore the lost endocrine function, meaning you might still end up as a brittle diabetic. Which explains why we try every single lifestyle and medical intervention before letting a surgeon pick up the scalpel.