The Spectrum of Unresponsiveness: What Are We Actually Looking At?
Let us be clear about one thing. A person slumped on a sidewalk is not necessarily a textbook medical emergency, but treating them as a minor inconvenience is a gamble nobody should take. Consciousness is not a simple on-off switch; it is a complex neurological sliding scale. When we talk about how to deal with an unconscious person, we are analyzing a brain that has temporarily or permanently lost its ability to maintain awareness of its surroundings. In the medical field, this is often quantified using the Glasgow Coma Scale, which evaluates eye, verbal, and motor responses, but out in the real world, you do not have time for a numerical scoring system.
The Fine Line Between Syncope and a Comatose State
Fainting—or vasovagal syncope, if you want to get technical—is a transient loss of consciousness followed by a rapid, spontaneous recovery. It is usually harmless, caused by a sudden drop in blood pressure or a surge in vagal nerve activity. But where it gets tricky is differentiating that brief system reboot from a deep, prolonged comatose state induced by trauma, stroke, or a severe drug overdose. Statistics from the American Heart Association show that roughly 350,000 out-of-hospital cardiac arrests occur annually in the United States alone, and nearly all of them look like a simple faint in the first ten seconds. Can you spot the difference instantly? Honestly, it is unclear without checking the airway, and assuming someone is just resting is the fastest way to facilitate a tragedy.
Why the Human Brain Decides to Pull the Plug
The mechanisms behind a sudden collapse are diverse, ranging from profound hypoxia to metabolic failures like severe hypoglycemia. If you look at the emergency admissions data from Cook County Hospital in 2024, nearly 18% of unexplained unresponsiveness cases in urban centers linked back to accidental toxicological events, while another substantial chunk stemmed from undiagnosed cardiovascular anomalies. The brain demands roughly 20% of the body’s total oxygen supply despite accounting for only two percent of its weight. When that supply line gets choked off, the cerebral cortex shuts down non-essential functions to preserve the brainstem. That changes everything for the responder because a limp body cannot protect its own airway.
Immediate Tactical Assessment: The First Thirty Seconds on the Scene
Forget everything you have seen on television dramas. Do not slap the person, do not throw cold water on their face, and please, under no circumstances, should you try to force liquid down the throat of someone who cannot swallow. The initial approach must be methodical, swift, and entirely devoid of emotional panic.
Securing the Perimeter and Reading the Visual Cues
Before you even touch the individual, look around. Is there a downed power line nearby? An empty pill bottle? The smell of volatile organic compounds? If you become a casualty yourself, the number of victims doubles and the system breaks. Once the environment is deemed safe, you check for responsiveness by kneeling down, shaking their shoulders firmly, and shouting loudly. I have seen well-meaning people spend minutes trying to find a radial pulse in a wrist, which is a massive waste of precious time when the carotid artery in the neck is far more reliable. Yet, even the carotid pulse can be notoriously difficult to detect if your own adrenaline is pumping at maximum capacity.
The Deceptive Illusion of Agonal Breathing
This is where people don't think about this enough. Sometimes an unconscious person will make sporadic, gasping, or snoring noises that sound vaguely like breathing. This is not respiration; it is agonal breathing, a reflex originating from a dying brainstem that occurs in up to 40% of cardiac arrest victims during the initial minutes. If you mistake these guttural groans for normal breathing, you will withhold the chest compressions they desperately need, which explains why survival rates plummet when untrained bystanders manage the scene alone. Unless the chest is rising and falling rhythmically at least twelve times a minute, you must assume they are not breathing effectively.
The Physics of Airway Management and Positioning
When a human being loses consciousness, the muscles in their jaw relax completely. Contrary to the old urban legend, people cannot actually swallow their own tongue—anatomically, it is physically attached to the floor of the mouth—but the tongue does drop backward against the pharynx, functioning as a highly effective, lethal anatomical plug.
The Head-Tilt, Chin-Lift Technique Explained
To bypass this obstruction, you need to alter the geometry of the upper airway. By placing one hand on the forehead and the fingertips of your other hand under the bony part of the lower jaw, you tilt the head back gently while lifting the chin forward. This simple mechanical lever action pulls the tongue away from the back of the throat. Because the human airway is essentially a flexible tube, even a slight misalignment can completely restrict airflow, hence the need for precision. But what if you suspect a cervical spine injury from a fall on a concrete pier in San Francisco, or an automobile accident on Route 66? In those specific scenarios, the head-tilt is dangerous, and medical professionals utilize a jaw-thrust maneuver without moving the neck, a technique that requires significant practice to execute flawlessly.
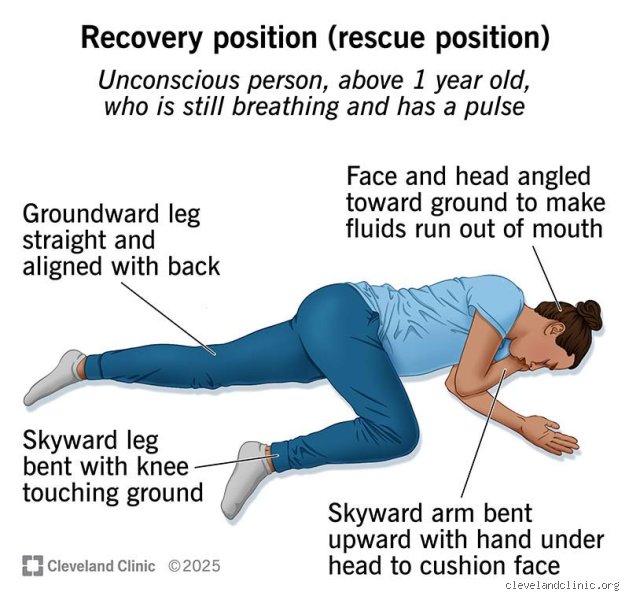
The Recovery Position: Keeping the Airway Clear
If the person is breathing normally but remains unresponsive, you cannot leave them flat on their back. What happens if they vomit? Without protective airway reflexes, they will aspirate that fluid directly into their lungs, leading to asphyxiation or a severe case of chemical pneumonia. The recovery position solves this by using the person's own limbs as levers to roll them onto their side, ensuring the mouth faces downward so fluids can drain freely. Except that you must ensure the top leg is bent at a right angle to anchor the body and prevent them from rolling onto their stomach. It is a simple, elegant piece of biomechanical engineering that has saved countless lives since its standardization by international resuscitation councils.
Comparing Interventions: Cardiopulmonary Resuscitation Versus Defensive Monitoring
Deciding when to transition from passive monitoring to aggressive intervention is a critical fork in the road when determining how to deal with an unconscious person. If you misjudge the situation, you risk causing harm, though the alternative of doing nothing is almost always worse.
When to Hold Back and Monitor
If the individual has a strong, regular pulse and is breathing clearly, your job is purely defensive. You call emergency services, place them in the recovery position, keep them warm, and watch them like a hawk. You do not leave them to go find a glass of water. The issue remains that an apparently stable unconscious patient can deteriorate into full arrest in a matter of seconds. As a result: your eyes must never leave the rise and fall of that chest until the paramedics take over the scene.
The Reality of Hands-Only CPR for Responders
If there is no breathing or only agonal gasps, you must begin chest compressions immediately. The medical paradigm has shifted dramatically over the past two decades toward hands-only CPR for untrained bystanders, eliminating the mouth-to-mouth component entirely for adult victims. Why? Because the blood remains oxygenated for several minutes after collapse, and the primary objective is maintaining the perfusion pressure required to send that remaining oxygen to the brain and myocardium. You need to push down hard—at least 2 inches deep—and fast, aiming for a tempo of 100 to 120 compressions per minute, which matches the rhythm of the classic song "Stayin' Alive." It is grueling, exhausting work that will likely crack ribs, but we are far from worrying about skeletal fractures when a life is actively slipping away.
Common Blunders and Lethal Myths
The Slap Reflex and Chemical Resuscitation
Forget cinema. Splashing freezing water on an unresponsive individual accomplishes absolutely nothing except lowering their core body temperature. Do not shake a comatose person violently under any circumstances. You might aggravate a hidden, brittle cervical spine fracture. Another classic, dangerous error involves shoving smelling salts or ammonia capsules under the nose of someone who cannot protect their airway. Why? Because the sudden, involuntary head jerk caused by the noxious fumes can instantly snap spinal structures. The issue remains that adrenaline-fueled bystanders often prioritize drama over basic clinical physiology.
The Tongue Swallowing Delusion
Let's be clear: nobody literally swallows their own tongue. That is physically impossible due to the frenulum anchoring it to the floor of the mouth. Yet, in an unconscious patient, the massive loss of muscular tone causes the tongue base to flaccidly slide backward, entirely occluding the pharynx. Never stick your fingers into the mouth of an inert casualty to grab this muscle. What happens instead? Their jaw muscles can spasm, clamping down and severing your digits while pushing the obstruction deeper. A simple head-tilt, chin-lift maneuver bypasses this entire anatomical nightmare safely.
Misreading Agonal Gasps as Normal Breathing
This is where fatal hesitation manifests. A person dying from sudden cardiac arrest might exhibit sporadic, reflexive snorting noises for up to several minutes. This is not respiration; it is a brainstem reflex called agonal breathing. If you mistake these sporadic, dying gasps for peaceful slumber, you will delay cardiopulmonary resuscitation. A flatline requires chest compressions, period. Except that panic frequently blinds the untrained eye to this subtle distinction, which explains why so many victims perish while bystanders simply watch and wait.
The Silent Threat: Positional Asphyxia in Public Spaces
When the Environment Suffocates the Patient
Medical textbooks love clean, empty floors. Real life is messy, cramped, and chaotic. When managing an unconscious person in a tight space like a crowded transit bus, a narrow bathroom stall, or a cluttered concert venue, the immediate physical surroundings present an invisible hazard. Positional asphyxia occurs rapidly when the trunk of an inert body is folded forward or compressed, preventing the diaphragm from expanding. Did you know that a slumped torso can reduce oxygen saturation to critical levels in under ninety seconds? It is terrifying. If the chest cannot rise freely because it is wedged against a porcelain toilet bowl or a car dashboard, the prognosis plummets.
Mechanical Optimization of the Space
You must actively manipulate the architecture around the casualty if extraction is impossible. Dragging a heavy body requires leverage, not brute force. Clear away chairs, backpacks, and debris within a two-meter radius immediately. If you are operating on soft surfaces like a plush mattress or a deep mud patch, the force of your chest compressions will merely sink the victim further into the ground rather than compressing the heart. Slide a rigid board, a wide baking sheet, or even a sturdy coffee table book underneath their shoulder blades. As a result: your mechanical force actually reaches the thoracic cage instead of being absorbed by memory foam.
Frequently Asked Questions
How long can the brain survive without oxygen during an unresponsive episode?
The neurological countdown triggers the exact millisecond normal systemic perfusion ceases. Cellular death within the cerebral cortex initiates between four to six minutes of total oxygen deprivation. By the time a down-time counter reaches ten minutes, irreversible encephalopathy or global brain death becomes a near mathematical certainty for 85% of victims. This razor-thin window is why immediate bystander intervention dictates survival outcomes long before paramedics arrive on the scene. Can we honestly afford to wait for the sirens while those precious seconds tick away?
Should I perform CPR if the individual is completely motionless but still breathing?
No, you should absolutely not compress the chest of someone who maintains an active, rhythmic pulse and clear respiration. Instead, your immediate priority shifts to safeguarding their airway by rolling them gently into the lateral recumbent recovery position. This specific anatomical posture relies on gravity to drain vomitus or blood safely out of the mouth, preventing fatal aspiration pneumonia. Monitor their chest rise continuously every thirty seconds until professional medical personnel assume control of the scene. But keep your hands poised for compressions, because an unstable unconscious person can deteriorate into full cardiac arrest without warning.
What if I accidentally break the ribs of an unresponsive individual while helping?
Fracturing a rib or separating the costal cartilage is an incredibly frequent side effect of high-quality manual chest compressions, occurring in roughly 30% of successful resuscitations. A fractured rib heals perfectly fine in a living patient, whereas a pristine skeletal structure is entirely useless to a corpse. The alternative to aggressive, deep compression depth is death. Good Samaritan laws globally shield well-intentioned rescuers from civil liability stemming from these exact types of incidental physical injuries sustained during emergencies. In short, push hard, push fast, and ignore the audible pops under your palms.
A Defiant Mandate for Active Intervention
We must dismantle the paralyzing culture of bystander hesitation that currently dominates public emergencies. Gazing at an unconscious person while recording video on a smartphone is a moral and societal failure. Human life is structurally fragile, yet it is incredibly resilient when met with immediate, assertive physical intervention. Your hands possess the literal mechanical power to sustain a stranger's cerebral metabolism. Stop waiting for a perfect, clean scenario or a permission slip from the universe. (You will never get one anyway). Step up, clear the airway, compress the chest forcefully, and actively drag that human being back from the brink of extinction.