The Diagnostic Mirage: When Clear Images Lie to Clinicians
Picture this: you are doubled over in a hospital ER in Boston, clutching your upper abdomen as if holding your organs inside, yet the glowing monitor shows a pristine, textbook-perfect pancreas. It happens more often than ER docs care to admit. The pancreas, that comma-shaped organ tucked quietly behind your stomach, regulates everything from blood sugar to fat digestion. But when its own digestive enzymes turn inward—a cannibalistic process known as auto-digestion—the resulting firestorm doesn't always leave immediate structural scars.
The Trap of the Acute Phase
But why the discrepancy? In the first 24 to 48 hours of an attack, the inflammatory cascade might only exist at a cellular level, rendering it invisible to standard radiography. I have seen clinicians dismiss agonizing epigastric pain simply because a computer screen refused to cooperate. We are far from a perfect diagnostic world, and a normal CT scan merely captures anatomy, not function. If the interstitial fluid hasn't accumulated enough to alter the organ's physical contour, the scan reads as clear. And that changes everything for a patient begging for pain management.
The Fallibility of the Revised Atlanta Classification
Medical consensus actually accounts for this visual delay, except that many frontline providers forget the rulebook under pressure. According to the Revised Atlanta Classification guidelines, establishing a diagnosis requires meeting two out of three specific criteria: characteristic abdominal pain, serum lipase or amylase levels elevated at least three times the upper limit of normal, and characteristic findings on cross-sectional imaging. Notice the math there? You only need the pain and the bloodwork. The scan is entirely optional for a definitive diagnosis, yet it remains an obsessive gatekeeper in modern triage culture.
Where It Gets Tricky: The Secretive Nature of Chronic and Mild Cases
If acute attacks can hide behind clean imaging, chronic pathology is downright invisible. Chronic pancreatitis involves a slow, smoldering burn that erases organ function over years. In its infancy, this persistent inflammation leaves the global architecture of the pancreas completely intact, making a standard contrast-enhanced CT practically useless.
The Early-Stage Chronic Conundrum
A landmark study published in the journal Gastroenterology tracked patients presenting with unexplained fatty stools and persistent back pain. The shocking revelation? Nearly 35% of individuals eventually diagnosed with early-stage chronic pancreatitis had completely normal initial CT scans. People don't think about this enough; structural changes like calcification, ductal dilation, and parenchymal atrophy are end-stage markers. Expecting a CT scan to catch early chronic pancreatitis is like expecting an X-ray to detect a microscopic stress fracture the minute it occurs. Honestly, it's unclear why we still treat the CT as an infallible oracle in these subtle scenarios.
The Interstitial Edematous Variant
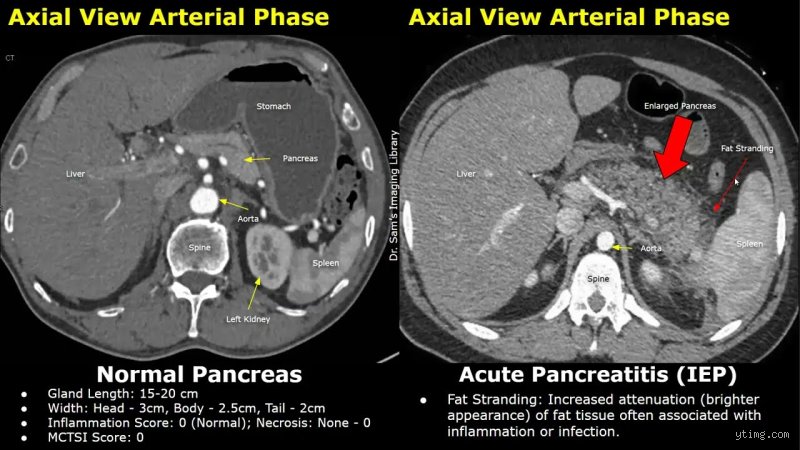
Even within acute classifications, the specific subtype dictates what the camera sees. Interstitial edematous pancreatitis is the milder, far more common variant, accounting for roughly 80% of all acute episodes. Because this form involves diffuse swelling rather than tissue death, it frequently evades the contrast thresholds of standard scanning equipment. A patient can be writhing in a hospital bed in Chicago with legitimate interstitial inflammation while their radiology report reads "unremarkable pancreas." Which explains why relying on a single modality creates a false sense of security among attending physicians.
Biochemical Reality vs. Radiographic Illusions
When the eyes fail, the blood usually tells the real story. The pancreas produces digestive enzymes that, under normal circumstances, remain dormant until they reach the duodenum. When pancreatitis strikes, these enzymes leak directly into the bloodstream, offering a biochemical signature that no normal CT scan can erase.
The Unforgiving Timeline of Serum Lipase
Serum lipase is the gold standard of pancreatic biomarkers, far outperforming its older sibling, amylase, in both sensitivity and specificity. Lipase levels typically peak within 24 hours of symptom onset and can remain elevated for up to two weeks. A patient might present with a pristine CT scan but possess a serum lipase count of 1,500 U/L against a normal ceiling of 50 U/L. Does the clear scan negate the chemical reality? Absolutely not. As a result: savvy gastroenterologists prioritize the laboratory trends over the pictures every single time, treating the patient's biochemistry and physical agony as the primary source of truth.
The Distraction of Hypertriglyceridemia
Here is an unexpected comparison: diagnosing pancreatitis via imaging alone is like trying to diagnose a engine failure solely by looking at the car's hood. What if the root cause is metabolic? In cases of hypertriglyceridemic pancreatitis—where serum triglycerides skyrocket past 1,000 mg/dL—the excess fat in the blood can actually interfere with both laboratory assays and contrast visualization. This lipid interference masks the severity of the inflammation, creating a double whammy of normal-looking labs and ambiguous scans that can delay life-saving plasmapheresis.
Beyond the Standard Scan: Alternative Diagnostic Weapons
When the standard CT draws a blank but clinical suspicion remains sky-high, the medical team must pivot to more sophisticated diagnostic weaponry. The issue remains that these advanced modalities are rarely available in an emergency room setting at three o'clock in the morning.
The Precision of Endoscopic Ultrasound (EUS)
Where the CT scan looks from the outside through layers of fat, muscle, and bowel gas, an Endoscopic Ultrasound gets up close and personal. By threading a specialized echoendoscope down the esophagus and into the stomach, a gastroenterologist can position the ultrasound transducer mere millimeters from the pancreatic parenchyma. This extreme proximity allows for the visualization of minimal change pancreatitis, detecting subtle ductal abnormalities and minor fibrotic strands that a CT scanner completely glosses over. It is the undisputed heavyweight champion for diagnosing early chronic changes, yet experts disagree on its utility during a raging, acute attack due to perforation risks.
Magnetic Resonance Cholangiopancreatography (MRCP)
Another heavy hitter is the MRCP, a non-invasive MRI protocol specifically tuned to evaluate the biliary and pancreatic ducts. While a CT scan is excellent for spotting gross tissue death, the MRCP excels at finding the underlying provocateur, such as a microscopic gallstone lodged deep within the common bile duct. But even this advanced technology has its limits; a tiny 2-millimeter biliary stone can easily hide from the magnetic fields if localized fluid accumulation causes too much artifact interference.