Understanding the Pancreas: Why This Hidden Organ Holds the Keys to Recovery
Tucked neatly behind your stomach lies a oblong, spongy gland that people rarely think about until it threatens their very survival. The pancreas is a dual-purpose workhorse. It pumps out insulin directly into your bloodstream to regulate glucose, while simultaneously manufacturing a heavy-duty cocktail of digestive enzymes, including trypsinogen, chymotrypsinogen, and lipase, which shatter the food you eat into absorbable nutrients. It is a flawless system. Except when the plumbing backs up.
The Spark of Autodigestion
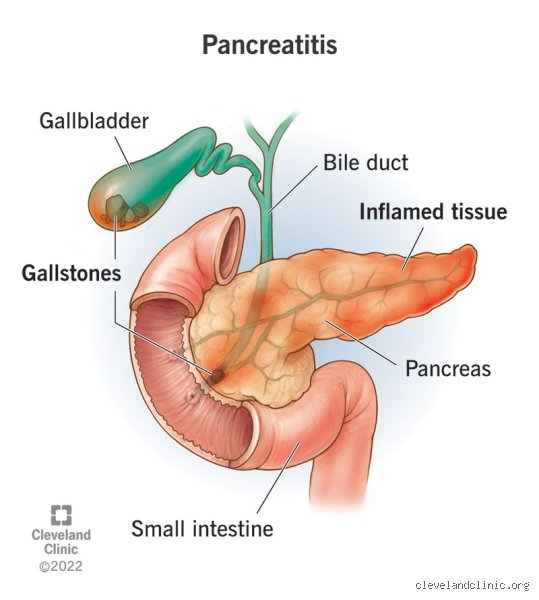
Pancreatitis is not a standard bacterial infection; rather, it is a civil war where the organ literally begins to digest itself. Normally, those potent enzymes remain completely inactive until they reach the duodenum. But when a rogue gallstone blocks the pancreatic duct at the Ampulla of Vater, or when a sudden surge of metabolic toxins from heavy alcohol intake disrupts the delicate cellular membranes, these enzymes activate prematurely inside the acinar cells. That changes everything. The resulting chemical burn triggers a massive influx of inflammatory cytokines, causing acute pancreatic necrosis, which can quickly spiral into a systemic medical emergency.
Acute Pancreatitis Cures: Medical Realities of Total Organ Regeneration
Here is where the biology offers some genuinely good news. The human pancreas possesses a remarkable capacity to heal from a single, isolated insult, provided the underlying trigger is permanently removed. In roughly eighty percent of acute cases, the inflammation remains interstitial and mild, meaning the cellular scaffolding stays intact. Patients typically endure a brutal three-to-five-day hospital stay characterized by aggressive intravenous hydration, stringent pain management, and complete bowel rest. And then? The pancreas simply resets, regenerates its lost acinar mass, and returns to baseline functioning without a single trace of long-term scarring.
The Dangerous Reality of Necrotizing Attacks
But what about the remaining twenty percent? That is where it gets tricky. In severe cases, the lack of blood flow causes actual tissue death, creating pockets of infected debris that doctors refer to as walled-off pancreatic necrosis. I have seen patients spend months in the intensive care unit battling multi-organ failure because of this specific complication. Yet, even in these extreme scenarios, a clinical cure is entirely possible through modern, minimally invasive interventions.
Consider the landmark PANTER trial published in The Lancet in 2010, which completely revolutionized how gastroenterologists approach this crisis. Instead of rushing patients into open abdominal surgery to hack away dead tissue, teams at academic centers like the Amsterdam University Medical Center pioneered the "step-up approach." This protocol uses percutaneous drainage followed, if necessary, by endoscopic necrosectomy to clear out dead matter through the stomach wall. By avoiding major surgery, the surrounding, healthy pancreatic tissue is spared. The patient recovers, the remaining organ tissue hypertrophies to compensate for the loss, and the individual is functionally cured, albeit with a slightly lower reserve capacity.
The Ultimate Prophylaxis: Eradicating the Root Cause
A true cure requires a permanent solution to the initial insult, which means addressing the biliary system. If ultrasound imaging reveals that a tiny, jagged five-millimeter gallstone migrated down the common bile duct and sparked the attack, the long-term solution is straightforward. Surgeons will perform a laparoscopic cholecystectomy during the same hospital admission. By removing the gallbladder, you eliminate the factory that produces the stones, thereby dropping the recurrence rate of acute biliary pancreatitis from nearly thirty percent down to less than two percent. The threat is gone.
Chronic Pancreatitis: Why Damage Control Replaces the Word Cure
When the inflammation becomes a repetitive, unrelenting loop, the conversation shifts from total eradication to aggressive damage control. Chronic pancreatitis is characterized by permanent, progressive morphological changes. The healthy, elastic parenchyma of the organ is gradually replaced by dense, fibrotic scar tissue, a grim process orchestrated by activated pancreatic stellate cells reacting to chronic oxidative stress.
The Point of No Return in TIGAR-O Classification
Clinicians use the TIGAR-O classification system to categorize these permanent cases based on toxic-metabolic, idiopathic, genetic, autoimmune, or obstructive risk factors. Think of the chronic form like liver cirrhosis or advanced pulmonary fibrosis; once the functional architecture is destroyed, no amount of medication can regrow those delicate, enzyme-producing factories. People don't think about this enough when managing early symptoms. By the time a patient presents with classic steatorrhea, which is foul-smelling, oily stools caused by fat malabsorption, the organ has already lost over ninety percent of its exocrine capacity. The cells are gone, replaced by calcified stones that plug the main pancreatic duct like tiny chunks of concrete.
The Autoimmune Exception: A Treatable Form of Chronic Dysfunction
Yet, there is one fascinating scenario where conventional medical wisdom about chronic disease is turned completely on its head. Autoimmune pancreatitis, specifically Type 1, which is a systemic fibroinflammatory disease mediated by IgG4-positive plasma cells, can look identical to pancreatic cancer on a standard CT scan. It presents with a classical "sausage-shaped" enlargement of the gland and strictures of the biliary tree. It looks utterly hopeless. Except that it isn't.
The Dramatic Corticosteroid Reversal
Is it truly cured? Well, we are far from a genetic reset, but the clinical response is nothing short of miraculous. When doctors administer a high-dose regimen of oral prednisone, typically starting at forty milligrams per day, the intense inflammatory infiltrate melts away within weeks. The strictures open up, the pancreatic duct decompresses, and exocrine function often rebounds significantly. It requires long-term maintenance therapy with immunomodulators like azathioprine to prevent relapses, but for this specific subset of patients, the disease can be forced into a profound, long-lasting remission that feels exactly like a cure.
Common mistakes and misconceptions about treating the pancreas
People love simple narratives, except that biology rarely obliges. The single biggest blunder we witness in clinical settings is the dangerous assumption that a temporary reprieve from agony equals a permanent victory. When the searing abdominal pain of an acute episode fades, patients frequently assume they are completely out of the woods. They are not. A damaged pancreas remains highly vulnerable for weeks, meaning that a premature return to greasy comfort foods can instantly trigger a violent relapse. Healing is a grueling marathon, not a sprint.
The myth of the absolute cure
Can pancreatitis be cured? If we are talking about the acute variant caused by temporary gallstone blockages, surgical removal of the gallbladder often resolves the root threat entirely. But applying this definitive logic to the chronic version is a grave error. Chronic pancreatic inflammation causes irreversible structural scarring. You cannot un-ring that bell. Believing that a handful of supplements or a trendy herbal detox can magically regenerate dead acinar cells is a fantasy. It delays actual medical management, which explains why so many patients present with advanced complications that could have been mitigated earlier.
The alcohol misconception and social stigma
Let's be clear: alcohol is not the solitary villain here. While heavy drinking accounts for roughly 40% of chronic cases, a massive chunk of diagnoses stems from genetic mutations, autoimmune responses, or hypertriglyceridemia. Assuming every patient brought this upon themselves via excessive drinking is a toxic stereotype. This stigma forces many individuals into deep denial, causing them to hide symptoms out of sheer embarrassment. Consequently, they miss the critical window for early therapeutic intervention.
The silent threat of exocrine pancreatic insufficiency
Medical conversations usually revolve around pain management, yet the issue remains that the organ's digestive duties are equally vital. When inflammation destroys more than 90% of the enzyme-producing tissue, a secondary condition called Exocrine Pancreatic Insufficiency, or EPI, rears its head. It is a stealthy assassin of quality of life.
Why malabsorption goes unnoticed until it is severe
Your body possesses remarkable backup systems. Because of this built-in redundancy, you might lose over half of your pancreatic function without experiencing a single noticeable symptom. But once the threshold is crossed, the consequences are stark. Fat-soluble vitamins vanish from your system unabsorbed, which leads to rapid weight loss, brittle bones, and foul-smelling, floating stools. Treating this requires precise pancreatic enzyme replacement therapy, administered with every single meal and snack. It is an exacting, lifelong regimen. (Many patients fail to realize that taking these capsules even a few minutes too late renders them entirely useless.)
Frequently Asked Questions
Can pancreatitis be cured completely if it is caused by gallstones?
Yes, acute biliary episodes offer the highest probability of a total clinical resolution. When a gallstone blocks the pancreatic duct, it triggers an immediate, volatile inflammatory cascade that accounts for approximately 35% to 40% of all acute admissions worldwide. Once a surgeon removes the gallbladder via cholecystectomy, the primary mechanical trigger is permanently eliminated. This intervention prevents future blockages in the vast majority of cases, allowing the pancreatic tissue to heal fully over the subsequent months. However, if the initial attack was severe enough to cause extensive necrotizing tissue damage, some localized permanent scarring may still persist despite the removal of the stones.
How long can a person live after being diagnosed with chronic pancreatic inflammation?
A diagnosis of chronic pancreatic disease is undoubtedly life-altering, but it is by no means an immediate death sentence. Studies indicate that the 10-year survival rate stands near 70%, while the 20-year survival rate hovers around 45% to 50%, with outcomes heavily dictated by lifestyle modifications. Individuals who completely cease all alcohol consumption and tobacco use experience significantly lower mortality rates compared to those who continue these damaging habits. The problem is that long-term inflammation slightly elevates the risk of developing pancreatic cancer, a factor that requires regular diagnostic surveillance. Ultimately, meticulous management of secondary complications like diabetes and malnutrition allows many patients to achieve a normal, robust lifespan.
Can dietary changes alone reverse the damage done to the pancreas?
Dietary modifications are incredibly powerful for symptom control, but they lack the biological capability to reverse existing fibrotic tissue damage. Adopting a strict regimen that caps daily fat intake at a maximum of 30 to 50 grams is vital to prevent overstimulating the organ. This nutritional framework minimizes painful flare-ups and reduces the workload on a struggling digestive system. And can a perfect diet replace prescription