Understanding the Basics of Permanent Birth Control and Why It Matters
When we talk about being sterilised, we are generally looking at two distinct surgical paths: tubal ligation for individuals with uteruses and vasectomy for those with testes. In the female procedure, a surgeon blocks or removes the fallopian tubes to prevent the egg from meeting the sperm. For men, the vasa deferentia—the tubes carrying sperm from the testicles—are severed. It sounds foolproof on paper, yet people don't think about this enough: surgery is performed by humans on living tissue, and living tissue is notoriously unpredictable. I have reviewed clinical files where patients were utterly blindsided by a positive test strip a decade after their procedures, proving that "permanent" is sometimes a relative term in medicine.
The Anatomy of a Supposedly Closed Road
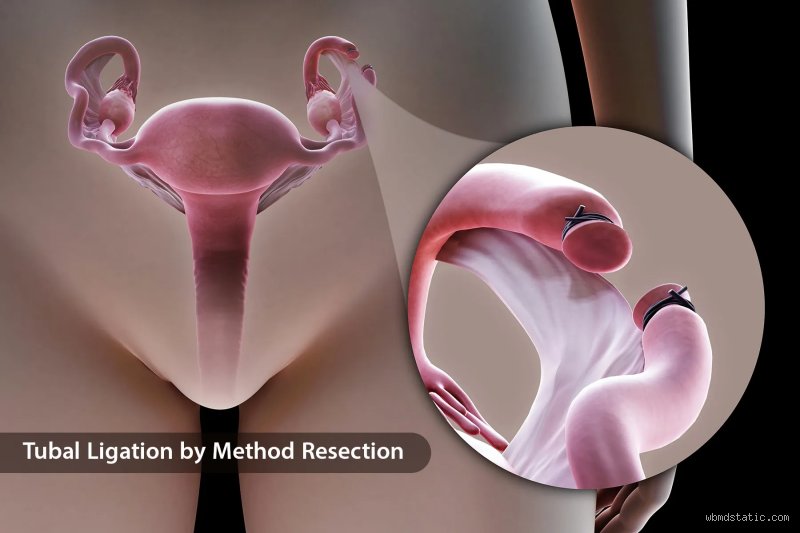
To grasp how this happens, we need to look at what happens post-op. In a standard bilateral tubal ligation, the fallopian tubes are disrupted using bipolar coagulation, silicone bands, or titanium clips like the Filshie system. The goal is complete occlusion. Except that sometimes, the body decides to initiate a process called recanalization. This is where microscopic channels form within the scar tissue, creating a tiny, hidden tunnel just wide enough for a single sperm to navigate. If that happens, that changes everything you thought you knew about your reproductive status.
The Statistical Reality of Surgical Failure
Let's talk numbers because the historical data presents a much more nuanced picture than the glossy brochures in your OB-GYN’s waiting room. The benchmark U.S. Collaborative Review of Sterilization (CREST) study remains the most comprehensive data set we have on this topic. Investigators tracked thousands of women over 14 years and discovered that the cumulative failure rate for all tubal sterilization methods combined was roughly 18.5 per 1,000 procedures. That is nearly a two percent chance over a decade. Honestly, it's unclear why some bodies heal with such aggressive persistence while others don't, but the data does not lie. Age at the time of surgery plays a massive role here; younger patients face a significantly higher cumulative risk of failure simply because their bodies have more years to attempt tissue repair.
How Your Body Can Undo a Tubal Ligation Over Time
Where it gets tricky is the specific mechanism of failure. Recanalization isn't the only culprit when someone gets pregnant while sterilised. There is also the issue of technical error during the initial surgery, such as a clip being placed on the round ligament by mistake instead of the fallopian tube. It sounds egregious, but when viewing pelvic anatomy through a laparoscope under less-than-ideal conditions, structures can look remarkably similar. A 2012 review in a prominent gynecological journal highlighted that misplacement accounts for a small but notable fraction of early-onset failures.
The Nightmare Scenario: Ectopic Pregnancy Risks
When a tubal ligation fails, it does not usually result in a textbook pregnancy. Because the altered fallopian tube is damaged or partially blocked, a fertilized egg often gets stuck on its journey to the uterus. Which explains why a staggering 33 percent of pregnancies that occur after a tubal ligation turn out to be ectopic. This is a life-threatening medical emergency where the embryo implants inside the tube itself. If you have had your tubes tied and experience severe pelvic pain or abnormal spotting, you cannot just shrug it off as a bad period. Why risk waiting until a rupture occurs? You need an ultrasound immediately because an ectopic rupture can cause massive internal bleeding within hours.
Luteal Phase Pregnancy: The Pre-Existing Condition
Then there is the bizarre phenomenon known as a luteal phase pregnancy. This happens when a person is actually already pregnant at the exact moment they lie down on the operating table, but the embryo is so small that a standard pre-op urine screening fails to detect it. Dr. Sarah Jenkins, an obstetrician practicing in Chicago, documented a case in 2018 where a patient underwent a flawless laparoscopic sterilization three days after conceiving during ovulation. The surgery went perfectly, but the fertilized egg was already safely past the point of surgical disruption, nestled cozy in the uterine lining. As a result: a perfectly healthy, completely shocking baby was born nine months later.
Vasectomy Failures: When the Partner's Surgery Recovers
We cannot discuss whether you can get pregnant while sterilised without looking at the other half of the equation. Vasectomies are widely considered safer and more effective than tubal ligations, but they are far from immune to the laws of biology. In fact, early failure is relatively common if couples skip the post-procedure safety protocols. A vasectomy does not clear out the pipes instantly; sperm stored upstream in the seminal vesicles can remain viable for months.
The Crucial Three-Month Clearance Window
Clinical guidelines from the American Urological Association mandate that men must submit a semen sample for analysis roughly 12 weeks post-vasectomy or after at least 20 to 30 ejaculations. Until that lab report reads "azoospermia"—meaning zero live sperm are present—you are playing Russian roulette with your fertility. Yet, compliance is notoriously abysmal. Up to 40 percent of men fail to return for their follow-up testing, assuming that because the scalpel wounds have healed, they are sterile. They aren't. And that is precisely when surprises happen.
Late Recanalization in Men
But what about late vasectomy failure, occurring years down the road? This is the male equivalent of the fallopian tube healing itself. The severed ends of the vas deferens can occasionally form a granuloma—a knot of inflammatory tissue—which inadvertently acts as a bridge, allowing sperm to swim across the gap. The incidence is low, roughly 1 in 2,000 cases, but when it happens, the sperm count can suddenly rebound to fertile levels without any physical warning signs whatsoever.
Comparing Sterilization Methods to Long-Acting Reversible Contraception
Here is a sharp opinion that contradicts conventional medical wisdom: traditional tubal ligation is rapidly becoming obsolete, and frankly, it probably should be. For decades, we viewed surgical sterilization as the gold standard of birth control, the pinnacle of efficacy. Yet, modern Long-Acting Reversible Contraception (LARC) systems, like the levonorgestrel intrauterine device (IUD) or the subdermal etonogestrel implant, actually boast lower real-world failure rates than having your tubes tied. The failure rate for the hormonal implant is a microscopic 0.05 percent, compared to the roughly 0.5 percent first-year failure rate of certain tubal methods.
The Shift Toward Total Salpingectomy
Because of these sobering statistics regarding how people get pregnant while sterilised, the American College of Obstetricians and Gynecologists now heavily favors a different surgical approach: the bilateral salpingectomy. Instead of clipping or burning a small segment of the fallopian tubes, surgeons now prefer to remove the tubes entirely from the uterine cornua to the fimbriae. This radical shift, which gained massive traction between 2015 and 2022, serves a dual purpose. It drops the risk of subsequent pregnancy to practically zero—as there is no tube left to recanalize—and it simultaneously slashes the risk of epithelial ovarian cancer, which often originates in the fallopian tissue. It is a structural upgrade that renders old-school tubal ligation look like a crude relic of twentieth-century medicine.
Common mistakes and misconceptions
The myth of immediate bulletproof protection
You walk out of the surgical center, breathe a sigh of relief, and assume your reproductive chapters are permanently shuttered. Except that biology laughs at human impatience. For those undergoing a vasectomy, mobile swimmers linger in the upper anatomical plumbing for months. Failing to utilize backup contraception during this interim phase remains the primary driver of unexpected post-procedure conceptions. Even with tubal ligation, assuming instantaneous invulnerability can backfire if fertilization occurred mere hours before the clips were applied.
Conflating sterilization with absolute immunity
Let's be clear: surgical birth control is not a magical force field. People routinely conflate the concept of permanent contraception with an mathematical zero probability of conception. It is a logical fallacy that blinds individuals to early bodily changes. Because the mind deems pregnancy impossible, early symptoms like nausea or fatigue get attributed to food poisoning or stress, delaying critical medical evaluation.
Misunderstanding the body's aggressive healing capacity
We drastically underestimate human tissue. The problem is that the body views a surgically severed fallopian tube as an injury requiring intense repair. Through a process called recanalization, microscopic channels can forge a path right through scar tissue, stitching the divided ends back together. This anatomical stubbornness explains how you can get pregnant while sterilised years after a flawless operation.
The hidden reality of ectopic risks and expert guidance
The treacherous terrain of out-of-place implantations
When permanent birth control methods fail, they do not fail gracefully. If an egg somehow encounters a rogue sperm after a tubal procedure, the altered anatomy frequently prevents the resulting embryo from reaching the uterus. As a result: the pregnancy implants within the damaged fallopian tube itself, creating a life-threatening medical emergency. Every reproductive endocrinologist will tell you that a positive test after sterilization demands an immediate ultrasound to rule out this specific catastrophe.
Proactive vigilance over passive assumption
Do you actually know the signs of an ectopic rupture? Sharp unilateral pelvic pain or erratic spotting cannot be ignored under the assumption that your tubes are tied. Our medical limits mean we can never guarantee a 0% failure rate for any procedure. Experts strongly advocate for annual gynecological checkups where contraceptive integrity is openly discussed, rather than assuming a decade-old surgery remains structurally sound today.
Frequently Asked Questions
Can I get pregnant while sterilised years after the initial procedure?
Yes, because time does not diminish the slight statistical baseline risk of failure; in fact, long-term data indicates that cumulative failure rates can rise slightly over a decade. The landmark US Collaborative Review of Sterilization tracked thousands of patients and revealed that the 10-year cumulative failure rate for all tubal sterilization methods combined sits at approximately 18.5 per 1,000 procedures. Certain techniques, like bipolar coagulation, exhibited failure rates as high as 36.5 per 1,000 cases over that same ten-year window. Tissue recanalization or fistulous tract formations can occur at any point, meaning a woman who underwent surgery in her twenties might still face a surprise positive test in her late thirties.
What are the actual odds of experiencing a sterilization failure?
While the overall probability remains remarkably low compared to temporary methods like the pill or barrier options, it is never absolute. For vasectomies, the failure rate hovers around 0.15% after confirmed azoospermia, making it slightly more reliable than its female counterparts. Modern hysteroscopic micro-inserts, which have largely been phased out but remain inside millions of individuals, carried a failure rate near 0.1% to 1.1% depending on proper placement verification. Yet, the issue remains that these tiny percentages represent real individuals who navigate unexpected parental realities every single year.
How does an ectopic pregnancy manifest after a tubal ligation?
An ectopic pregnancy typically presents with abnormal vaginal bleeding coupled with severe, localized abdominal pain, often occurring six to eight weeks after a missed menstrual cycle. Statistics indicate that if a woman experiences a failure after a tubal sterilization, the probability that the pregnancy is ectopic skyrockets to roughly 33% of those total failures. This stands in stark contrast to the general population, where ectopic implantations account for a mere 2% of total conceptions. Immediate surgical intervention or medical management with methotrexate is mandatory to prevent internal hemorrhage and protect maternal health.
A definitive stance on permanent contraception realities
We need to dismantle the dangerous medical rhetoric that frames sterilization as an absolute, unquestionable guarantee. Medicine likes neat categorizations, but human biology prefers chaotic adaptation, which explains why the question of whether you can get pregnant while sterilised cannot be answered with a simple negative. Expecting absolute perfection from a surgical intervention ignores the realities of cellular regeneration. It is time for practitioners to stop downplaying the failure margins during pre-operative consultations. True reproductive autonomy requires patients to hold full awareness of these long-term statistical risks, ensuring they remain vigilant instead of blindsided by their own biology. Ultimate certainty is a comforting illusion, but clinical transparency saves lives.