The Structural Void: Understanding the Anatomical Shift in the Pelvic Floor
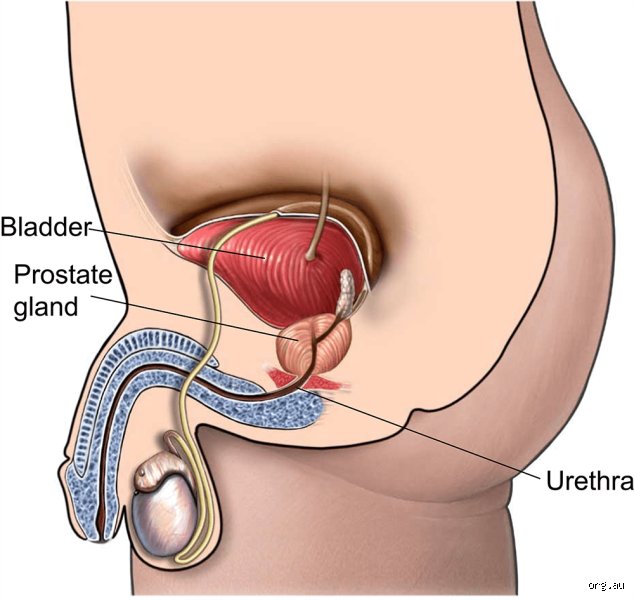
Once the surgeon extracts that small, troublesome piece of flesh—whether via the Da Vinci robotic-assisted system or a traditional open incision—your internal architecture undergoes a seismic shift. I believe we underestimate the sheer mechanical shock of this procedure. Imagine a bridge where the central pylon is suddenly yanked out; the remaining structures don't just sit there, they sag, stretch, and lean into the empty space. In the case of a radical prostatectomy, the bladder actually drops lower into the pelvis to connect directly to the remaining stump of the urethra. This isn't just a minor adjustment. It is a violent re-plumbing of your most private systems that forces the external urinary sphincter to take on a workload it was never designed to handle alone.
The Disconnection of the Vesicourethral Anastomosis
Where it gets tricky is at the junction called the anastomosis. Surgeons must stitch the neck of the bladder directly to the urethra (the tube you pee through) after the prostate is gone. But here is a reality check: those stitches are under constant tension because the bladder is being pulled into a position it hasn't occupied since you were a fetus. Because the internal urethral sphincter—which lived inside the prostate—is now in a biohazard bin, you are left relying entirely on the external version. Does the body always play ball? Not immediately. For the first few weeks, that connection is raw, inflamed, and prone to leaking under the slightest pressure from a cough or a laugh. Experts disagree on the "perfect" suturing technique, yet the result for the patient remains a period of significant mechanical instability that can last months.
The Neurological Gamble: Nerve-Sparing Techniques and the Reality of Potency
We often hear about "nerve-sparing" surgery as if it were a guaranteed insurance policy for your sex life, but honestly, it’s unclear how much "sparing" actually translates to function in the first two years. These nerves, known as the cavernous nerves, are microscopic threads that cling to the sides of the prostate like spiderwebs on a moving vehicle. Even if the surgeon’s blade doesn't touch them, the heat from cautery or the simple act of stretching them during the removal can cause what doctors call neuropraxia. This is essentially a "nerve stun" that puts your erectile capacity into a deep coma. And let’s be real: waiting eighteen months for a sign of life downstairs feels less like "recovery" and more like a test of psychological endurance that changes everything about how a man views his own masculinity.
The Role of Nitric Oxide and Tissue Oxygenation
When those nerves are dormant, the biology of the penis changes. Without regular signals from the brain to engorge with blood, the corpora cavernosa (the spongy chambers of the penis) suffer from a lack of oxygenated blood. This isn't just a "wait and see" situation. Over time, a lack of erections can lead to collagen deposition and fibrosis, which is a fancy way of saying the tissue scars and loses its elasticity. This explains why many modern clinics in cities like London or New York push for "penile rehabilitation" protocols involving PDE5 inhibitors like Sildenafil as early as two weeks post-op. As a result: the goal isn't necessarily a romantic encounter, but rather a desperate attempt to keep the plumbing from rusting shut while the nerves slowly wake up from their surgical slumber.
The Ghost of the Ejaculatory System
But the most jarring change for many is the permanent end of ejaculation. Since the seminal vesicles are typically removed along with the prostate, the factory that produces the fluid for semen is gone. You will experience what is known as a "dry orgasm." It feels the same—or close to it—but nothing comes out. Except that occasionally, some men experience climacturia, which is the involuntary leakage of urine during an orgasm. It is one of those medical side effects people don't think about enough until it happens in the heat of the moment, creating a psychological barrier that can be harder to heal than the surgical scars themselves.
The Urinary Paradox: Why the First 90 Days Are a Battle of Physics
Incontinence is the elephant in the room that every urologist mentions, yet few patients truly grasp the daily logistics until they are buying their first pack of heavy-duty pads. Statistics show that roughly 6% to 15% of men will deal with long-term leakage, but in that first 90-day window? The number is closer to 90%. Your body is fighting gravity. The weight of your abdominal organs is pressing down on a bladder that no longer has a prostate-shaped "shelf" to sit on. Hence, the frantic focus on Kegel exercises to beef up the levator ani muscles.
The Misunderstood Pelvic Floor Tension
The issue remains that most men do their Kegels wrong. They clench their glutes or hold their breath, which actually increases intra-abdominal pressure and makes the leaking worse. You have to isolate the muscles you'd use to stop a fart in an elevator, and you have to do it hundreds of times a day. We're far from it being a simple fix. In fact, over-training can lead to a hypertonic pelvic floor, where the muscles become so tight and fatigued they actually stop functioning, leading to a weird paradox of pelvic pain and increased incontinence. It is a delicate balance of strength and relaxation that requires the kind of body awareness most men haven't practiced since high school sports.
Comparing Radical Prostatectomy to Focal Therapies: A Modern Dilemma
For decades, the "gold standard" was to cut the whole thing out, but the 2024 EAU (European Association of Urology) guidelines have started to shift the conversation toward more nuanced approaches. If you compare a radical prostatectomy to something like HIFU (High-Intensity Focused Ultrasound) or Cryotherapy, the difference in "collateral damage" is staggering. Focal therapies aim to zap only the tumor, leaving the surrounding nerves and the urethral sphincter intact. Which explains why men are increasingly opting for these "middle ground" treatments, even if the long-term cancer recurrence data isn't as robust as the 20-year stats we have for surgery. The issue is a trade-off between the certainty of cancer removal and the certainty of maintaining a baseline quality of life.
The Radical Approach vs. Active Surveillance
Then there is the camp that argues we are over-treating. In 2012, the landmark PIVOT study suggested that for low-risk prostate cancer, surgery didn't significantly reduce mortality compared to observation over a 10-year period. This creates a massive psychological burden. Imagine being told you have "cancer" but that the best move is to do nothing, versus having an operation that might cure you but will definitely change how you pee and have sex forever. It’s a brutal choice. Yet, for those with aggressive, high-grade Gleason 8 or 9 tumors, the surgery isn't an option; it's a lifeline. In short, the "body" you have after the prostate is gone is a body that has traded its biological peak for a chance at a longer, albeit drier, future.
Shattering the myths: common mistakes and misconceptions
The problem is that many patients enter the surgical suite envisioning a binary outcome where they are either cured or broken. This is a reductive fallacy that ignores the biological gray zones of recovery. You might hear neighbors whisper that radical prostatectomy equates to an immediate, permanent end to all sexual vitality. Let's be clear: the "all-or-nothing" narrative is a lie. While the cavernous nerves responsible for erections are indeed sensitive to the trauma of retraction and heat during surgery, they often exist in a state of neuropraxia—a temporary slumber rather than a total severance. But if you wait two years to address it, the tissues may fibrose. Why do so many men suffer in silence when penile rehabilitation protocols, utilizing PDE5 inhibitors or vacuum devices, show a 40% to 60% higher success rate in regaining functional erections compared to "watchful waiting"?
The misconception of instant dryness
Another frequent blunder involves the timeline of urinary control. Many expect to be leak-free the moment the indwelling catheter is removed, typically 7 to 14 days post-op. This is unrealistic. Your internal urethral sphincter has just lost its primary neighbor and support structure. You will leak. However, thinking that Kegel exercises are a magic wand is equally dangerous; performing them incorrectly can actually fatigue the pelvic floor, leading to more "insult to injury" accidents. Statistics show that roughly 90% of men regain acceptable continence within 12 months, yet the first eight weeks are a chaotic landscape of damp pads and frustration. Except that we rarely discuss the "climax leak"—climacturia—where small amounts of urine escape during orgasm, a harmless but startling reality for nearly 40% of post-operative patients.
The "Cancer-Free" trap
We often see men abandon their health monitoring once the pathology report looks clean. That is a dangerous oversight. Because the prostate is removed, your Prostate-Specific Antigen (PSA) should ideally drop to undetectable levels, usually defined as less than 0.1 ng/mL. If you assume the battle is over, you might miss a biochemical recurrence. The issue remains that microscopic cells can linger. Constant vigilance via serial PSA testing is the only way to ensure the surgery actually achieved its curative intent.
The pelvic floor's hidden role and expert strategy
Beyond the obvious plumbing issues, there is a "silent" adjustment happening within your levator ani muscle complex. When the prostate is excised, the bladder actually drops slightly lower in the pelvis to be reattached to the urethra—a process called vesicourethral anastomosis. This repositioning changes the mechanical leverage of your entire lower abdomen. Yet, most surgical consults never mention the impact on bowel habits. The issue remains that your pelvic floor is now working overtime to support the bladder, which can lead to pelvic floor hypertonicity or paradoxical tension. You might feel a phantom sensation, a heaviness in the perineum that feels like sitting on a golf ball, even though the organ causing that sensation is long gone.
Expert advice: The pre-habilitation advantage
If you want to optimize what happens to your body once your prostate is removed, you must start before the first incision. Experts now advocate for "pre-hab"—a rigorous 4-week strength program for the pelvic muscles prior to surgery. (It is much harder to learn to find a muscle when it is screaming in post-operative pain). By building a neuromuscular reserve, you effectively provide your body with a safety net. Which explains why men who engage in pre-operative physical therapy often achieve dryness 3 to 5 months faster than those who start post-catheter. It is not just about strength; it is about proprioception, or the brain's ability to locate and squeeze the right valve under pressure.
Frequently Asked Questions
Will I still be able to produce semen during an orgasm?
No, you will experience what is medically termed a "dry orgasm" because the seminal vesicles and the prostate, which produce 95% of the ejaculate fluid, are gone. The sensation of climax remains centered in the nervous system and is usually just as intense, though the physical mechanics are forever altered. As a result: you will be biologically sterile, meaning natural conception is no longer possible without surgical sperm retrieval. For many, this is a psychological hurdle that requires more adjustment than the physical lack of fluid itself. Data suggests that 75% of men eventually adapt to this "new normal" without a significant loss in overall sexual satisfaction scores.
How long does the actual physical pain of recovery last?
The acute surgical pain from robotic-assisted laparoscopic incisions usually dissipates within 5 to 7 days, though internal soreness lingers. You will likely feel a deep pelvic ache for 2 to 3 weeks, especially when sitting or during bowel movements. But the most annoying discomfort is often the referred shoulder pain caused by the CO2 gas used to inflate the abdomen during the procedure. In short, while you might be walking a mile within a week, your body is performing cellular remodeling for at least six months. Most clinical guidelines suggest avoiding heavy lifting over 10 pounds for a minimum of six weeks to prevent incisional hernias.
Can I still get a "natural" erection without any pills or pumps?
The possibility of spontaneous erections depends heavily on whether the surgeon performed a nerve-sparing technique and your baseline function before the operation. If you were 100% functional before, there is a 60% to 80% chance of returning to "intercourse-grade" erections within 18 to 24 months. However, the timeline is agonizingly slow because nerves heal at a rate of only one millimeter per day. You must be proactive. Penile oxygenation is vital; if the penis does not receive regular blood flow through nocturnal erections (which stop after surgery), the tissue can shrink by 1 to 2 centimeters. This penile atrophy is a preventable tragedy if you utilize rehabilitation tools early and often.
The unvarnished truth: A synthesis
The removal of the prostate is not a return to your twenty-year-old self, nor is it a sentence to a life of diapers and celibacy. It is a fundamental recalibration of your masculine identity and biological function. I take the firm stance that medical stoicism is the enemy of a good recovery; the men who thrive are those who aggressively pursue physical therapy and sexual rehabilitation. We must stop treating the "side effects" as secondary concerns, because for the survivor, they are the primary reality of daily life. The surgery might save your life, but your proactive engagement is what saves the quality of that life. In short, your body will never be the same, and perhaps that is an opportunity to rebuild it with more intentionality and care than ever before. Success is measured not just by a zero PSA, but by the ability to laugh, move, and love without the shadow of the surgery Looming over every moment.