Where It Gets Tricky: Defining the Mechanics of a Thrombus and an Embolus
Let us strip away the sterile textbook jargon for a second. When you cut your finger while chopping carrots, your body relies on a cascade of proteins to form a localized plug—a thrombus. That is normal, life-saving physiology. But when a clot forms inappropriately inside your deep veins, usually deep within the calves or thighs, clinicians label this deep vein thrombosis, or DVT. Here is the twist: that stationary lump of blood is not a pulmonary embolism yet.
The Moment of Transformation
Everything changes when a piece of that deep vein clot breaks free. It becomes an embolus, a nomadic piece of biological debris drifting through the venous superhighway, passing right through the right side of the heart, and slamming directly into the pulmonary arteries. Doctors at the Mayo Clinic tracking these cardiovascular anomalies note that approximately 1 in 3 individuals with a DVT will eventually experience a migration event. It happens fast. One minute you are dealing with a dull ache in your leg, and the next, you are facing a massive vascular blockade. Is PE the same as a blood clot? Strictly speaking, a PE is the catastrophic destination, while the blood clot was merely the vehicle that took you there.
A Spectrum of Coagulation
People don't think about this enough, but clots manifest in various vascular territories with completely different outcomes. An arterial clot in the brain triggers an ischemic stroke, while one in the coronary arteries causes a myocardial infarction. A PE, conversely, is exclusively a venous-side disaster that ends up disrupting the respiratory system. The issue remains that we tend to use "blood clot" as a lazy, catch-all phrase, erasing the terrifying choreography involved when a thrombus detaches and morphs into a lethal pulmonary obstruction.
The Pulmonary Pipeline: Why Your Lungs Bear the Brunt of the Damage
To grasp why a PE is so uniquely perilous, you have to look at the pulmonary circulatory architecture, which acts like a massive, finely woven strainer. The right ventricle of your heart pumps oxygen-depleted blood directly into the pulmonary artery, which immediately branches into smaller and smaller vessels to wrap around the microscopic air sacs where gas exchange occurs. When a rogue clot arrives here, it wedges itself tightly into these narrowing tubes.
The Hemodynamic Domino Effect
What happens next is a brutal exercise in fluid dynamics. The physical blockage creates an immediate backup of pressure, forcing the right ventricle to labor frantically against a suddenly unyielding wall of resistance. Statistics from the American Heart Association indicate that acute right ventricular failure is the primary cause of death in severe PE cases, rather than a lack of oxygen itself. Yet, the public narrative always focuses on suffocation. It is a cardiovascular ambush masked as a lung problem. I honestly believe our public health campaigns fail miserably by focusing so much on leg swelling while ignoring how quickly the heart buckles under the strain.
When Ischemia Strikes the Lung Tissue
Because the clot prevents blood from reaching specific segments of the lung, those areas can undergo pulmonary infarction—actual tissue death from oxygen starvation. Imagine turning off the water supply to one specific quadrant of a garden; the plants wither within hours. In the human body, this translates to sharp, stabbing chest pains that mirror a heart attack. Except that, unlike a heart attack, the pain often intensifies the moment you try to take a deep breath, a classic pleuritic symptom that should immediately send anyone racing to the nearest emergency room.
The Clinical Footprint: How Doctors Identify a PE on the Ground
Diagnosing a pulmonary embolism is notoriously difficult because it loves to mimic other, less sinister conditions like panic attacks, asthma flares, or simple bronchitis. A patient walks into an emergency department in Chicago or London complaining of sudden shortness of breath and a racing pulse, and the medical team must immediately initiate a diagnostic scavenger hunt. They cannot just rely on a hunch.
The Diagnostic Toolkit
First comes the D-dimer test, a blood draw that looks for protein fragments left behind when a blood clot dissolves. If it is negative, doctors can usually breathe a sigh of relief and rule out a thromboembolic event entirely. But if it comes back elevated—which happens easily from something as simple as recent minor surgery or inflammation—the hunt intensifies. That changes everything. The gold standard then becomes the CT pulmonary angiograph, a specialized scan utilizing contrast dye to map out the pulmonary vasculature in exquisite, three-dimensional detail. If there is a filling defect where the dye cannot flow, the diagnosis is sealed.
A Compelling Comparison: The Clogged Fuel Line
Think of the pulmonary artery as the main fuel line of a high-performance engine. If a tiny speck of rust gets stuck in the fuel filter, the engine splutters but keeps running; if a massive chunk of debris blocks the main line, the whole system cuts out instantly. In medical terms, we call that a saddle embolism, a massive clot that sits right at the bifurcation of the main pulmonary artery, completely cutting off blood flow to both lungs simultaneously. As a result: sudden collapse, often without any prior warning signs whatsoever.
Distinguishing the Danger: Is PE the Same as a Blood Clot in Your Leg?
While a DVT in the lower extremity and a PE are two sides of the same pathophysiological coin—collectively known as venous thromboembolism—their immediate danger profiles are light-years apart. A clot sitting quietly in your femoral vein is a ticking time bomb, but it is not currently killing you. A PE, however, is an active detonation.
Contrasting Symptoms and Survival Realities
Let us look at how these two stages of the same disease process present themselves in a clinical setting:
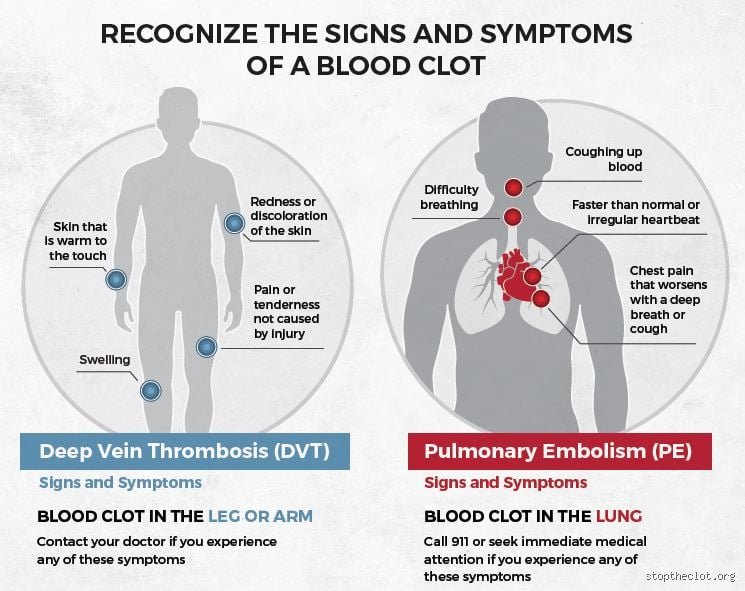
A deep vein thrombosis typically announces itself through unilateral leg swelling, warmth, and a distinct redness that feels like a severe muscle cramp that will not quit. Walk on it, and it burns. But when that identical clot migrates and becomes a PE, the symptoms instantly shift northward, presenting as unexplained shortness of breath, a rapid heart rate exceeding 100 beats per minute, and hemoptysis, which is the medical term for coughing up blood. The mortality rate for an untreated DVT is relatively low, but for an undiagnosed, massive PE, the mortality rate skyrockets to roughly 30 percent within the first few hours of symptom onset.
The Paradox of Safe Clots
Here is where nuance contradicts conventional wisdom: not all blood clots in the legs are destined for the lungs, and experts disagree on how aggressively to treat certain superficial clots. Clots that form in the veins just beneath the skin surface rarely migrate because they lack the massive muscular pumping action that surrounds the deep venous system. Hence, while a superficial clot causes discomfort and localized inflammation, it is generally considered benign compared to its deep-tissue cousins. We are far from a scenario where every single vascular clump requires a frantic rush to the ICU, yet patients panic equally for both because the internet uses the blanket term "blood clot" indiscriminately.