Understanding the Post-Surgical Landscape: Why the Drainage Bag Exists
When a surgeon performs a radical prostatectomy—the complete removal of the prostate gland—they are essentially performing a delicate plumbing overhaul. Because the prostate sits directly beneath the bladder and wraps around the urethra like a stubborn donut, its removal leaves a gap. Surgeons must pull the bladder down and reattach it to the urethral stump. This specific junction is called the vesicourethral anastomosis. If you tried to urinate normally through this fresh "suture line" immediately, the pressure would likely cause a leak or a total breakdown of the repair. But wait, why can't we just hold it? Because the body produces urine 24/7, and that fluid needs a low-pressure exit strategy while the stitches settle into place.
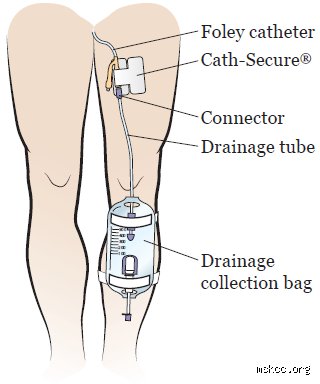
The Role of the Foley Catheter and Collection Systems
This is where the indwelling Foley catheter enters the picture. It is a flexible tube inserted through the penis that travels all the way to the bladder, held in place by a tiny water-filled balloon. People don't think about this enough, but that tube acts as a scaffolding for the new connection. It ensures that the bladder stays empty and decompressed. During your first week at home, you will typically switch between a larger "night bag" that hangs by the bed and a discreet "leg bag" that hides under your trousers. In short, the bag is just the reservoir; the catheter is the real workhorse. I find the common fear surrounding these bags stems from a lack of clear pre-op communication regarding the sheer temporary nature of the hardware.
Clearing Up the Stoma Confusion
Let’s be blunt: a prostatectomy bag is not a colostomy bag. There is a massive difference between a urinary catheter and an urostomy or colostomy, where a portion of the intestine is redirected to an opening in the abdominal wall. Unless your cancer has invaded the bladder or rectum to an extreme degree—a rarity in standard localized prostate cancer cases—you will not have a permanent bag attached to your stomach. The issue remains that the word "bag" carries a heavy psychological weight. Yet, for 98% of prostatectomy patients, the bag is gone before the two-week follow-up appointment. It’s a sprint, not a marathon.
Technical Mechanics of the Healing Process After Prostate Removal
The healing timeline is dictated by biology, not just the surgeon's skill. Within the first 48 hours, inflammatory responses peak at the site of the anastomosis. During this window, any internal pressure could cause urine to seep into the pelvic cavity, leading to a condition called a urinoma, which often requires further drainage. By day five, the mucosal lining of the bladder and urethra begins to fuse. This is a microscopic dance of cellular regeneration. Which explains why doctors are so insistent on the bag staying put; pulling it too early is like removing the cast from a broken leg while the bone is still soft. Some experts disagree on the exact day of removal—some push for day 7, others prefer day 14—but the consensus is that early removal increases the risk of strictures or scarring.
The Impact of Robotic vs. Open Surgery on Drainage
Does the type of surgery change the bag requirement? Not really. Whether you undergo a Robot-Assisted Laparoscopic Prostatectomy (RALP), which became the gold standard around 2010, or a traditional open retropubic approach, the plumbing remains the same. However, the robotic approach often allows for more precise suturing. Because the DaVinci surgical system provides 10x magnification, the surgeon can theoretically create a more watertight seal. As a result: some centers are now experimenting with "ultra-early" catheter removal at 48 to 72 hours, though this remains controversial. My stance is that the extra few days with the bag are a small price to pay for avoiding a secondary procedure to fix a leak. It’s better to be annoyed by a bag for a week than to deal with a bladder neck contracture for a year.
The Pressure Dynamics of a Healing Bladder
Think of the bladder as a muscular balloon. When it fills, it stretches; when it empties, it contracts. These movements are violent on a microscopic level for a fresh surgical wound. The drainage bag creates a zero-pressure environment. By keeping the bladder empty, the bag allows the pelvic floor muscles and the urinary sphincter to rest. Except that resting doesn't mean they aren't working; they are actually recalibrating to the absence of the prostate. Interestingly, some men find that they don't even feel the urge to go because the bag handles everything. It’s a strange, hands-off period where your body’s most basic function is essentially automated by medical-grade silicone.
Management of the Urinary Bag in the First 14 Days
Managing the bag is less about medical expertise and more about basic physics and hygiene. Gravity is your best friend here. If the bag is higher than your bladder, the urine will backflow, increasing the risk of a Urinary Tract Infection (UTI), which is the last thing you want while recovering. You’ll spend your first week post-op adjusting the straps of your leg bag, trying to find that sweet spot where it doesn't slide down your calf. It’s annoying. But compared to the alternative of internal scarring, it’s a manageable nuisance. We’re far from it being an invisible process, but with loose-fitting sweatpants, most people won't even know you're wearing one.
Preventing Catheter-Associated Infections
Sterility is the name of the game. You have a direct highway from the outside world into your bladder. Patients are usually instructed to clean the meatus—the tip of the penis—twice daily with mild soap and water. The issue remains that biofilms can form on the surface of the catheter if left too long. Data from the Journal of Urology (2023) suggests that roughly 5-10% of post-prostatectomy patients may develop a minor UTI, though most are easily cleared with a short course of Nitrofurantoin. Where it gets tricky is if the catheter becomes blocked by a small blood clot. If you stop seeing drainage in the bag, that is a genuine medical emergency, as the bladder will painfully distend against the fresh stitches.
Transitioning from the Night Bag to the Leg Bag
The switch is a psychological milestone. The night bag, which holds about 2000ml of fluid, is bulky and tethers you to the bed. But the leg bag—usually 500ml to 750ml—offers freedom. It allows you to walk around the block, which is vital for preventing deep vein thrombosis (DVT) after surgery. You'll learn the "valve flick" move to empty it in the bathroom, a skill you never thought you'd master. Is it glamorous? No. Is it functional? Absolutely. The bag is effectively your training wheels as you move toward a life without a prostate. Hence, the transition is more about regaining mobility than anything else.
Comparing the Bag to Immediate Continence Methods
Some might wonder if there are alternatives to the bag. Could we use a suprapubic catheter instead? This involves a tube placed through the lower abdomen directly into the bladder, bypassing the urethra entirely. While this avoids having a tube in the penis—which many men find preferable for comfort—it still requires a collection bag. A few surgeons at high-volume centers like Mayo Clinic have explored using temporary internal stents that dissolve, but these are not yet standard practice. The reality is that the external bag remains the safest and most reliable method for monitoring output and ensuring a dry surgical site.
Internal Stents vs. External Drainage
Internal stents are a flashy concept, but they have a major flaw: you can't easily tell if they are working. With a bag, you have visual confirmation. You can see the color of the urine—which will transition from a dark cranberry red to a light rose, and finally to clear yellow. This visual feedback is a strong clinical indicator of internal healing. If we used internal stents, we'd be flying blind. And because the risk of a "silent leak" is so high in the first week, the external bag provides a level of security that internal methods simply can't match. That changes everything when it comes to patient peace of mind during those first nervous nights at home.
The Psychological Weight of the Collection Bag
Honestly, the hardest part of the bag isn't the physical sensation; it's the assault on one's dignity. There is a specific kind of vulnerability in carrying your waste in a plastic pouch. I’ve spoken to patients who felt they couldn't leave the house, convinced every passerby could hear the slosh of liquid. But here is a reality check: nobody is looking at your shins. Most people are too absorbed in their own lives to notice a slightly bulky pant leg. Nuance is required here—while the bag is a "medical necessity," it is also a temporary badge of survival. You've just had a major cancer surgery; the bag is just the evidence that your body is busy putting itself back together.
Common urban legends and physiological blunders
The problem is that our collective imagination often confuses "prostate surgery" with "permanent disability," leading to the frantic search for external drainage systems that most men will never actually touch. Many patients walk into their pre-operative consultation convinced they are signing up for a lifelong relationship with a plastic bag strapped to their thigh. This is a mirage. Let's be clear: a radical prostatectomy involves reconnecting the bladder to the urethra, preserving the internal plumbing entirely. You are not receiving a urostomy. That particular surgical detour is reserved for bladder cancer patients where the entire reservoir is evicted. Yet, the misinformation persists because the immediate post-operative week requires a temporary foley catheter, which does, in fact, drain into a bag for a few days. Because the brain latches onto the most traumatic visual, men often mistake this seven-day guest for a permanent resident.
The confusion between incontinence and ostomy
Do you need a bag if you have your prostate removed? Not in the way a colon cancer patient might. But the nuance is often lost in translation. Some believe that if the sphincter muscle fails, a bag becomes the only fallback. The issue remains that the medical industry markets "disposable guards" and "briefs" so aggressively that they are conflated with surgical bags. In reality, modern robotic-assisted laparoscopic prostatectomy allows for such high-precision nerve sparing that the rate of total, unmanageable leakage is remarkably low. If you find yourself leaking, you wear a pad, not a collection pouch. And why would you choose a bulky external bag when physical therapy can retrain the pelvic floor?
Misunderstanding the temporary catheter phase
Expect a bag for exactly 5 to 10 days. That is the hard limit for the vast majority of cases. During this window, the surgical site—specifically the vesicourethral anastomosis—must heal without being stretched by a filling bladder. It is a period of forced rest. But once that silicone tube is pulled out, the bag goes into the trash forever. Except that some guys hear "catheter" and think "forever." It is a brief, albeit annoying, tactical necessity.
The hidden variable: The Artificial Urinary Sphincter (AUS)
Let's pivot to the rare scenario where "dryness" isn't achieved through Kegels or time. While you still don't need a bag if you have your prostate removed in this situation, you might opt for internal mechanical intervention. If 12 months pass and a patient is still using more than 3 heavy pads a day—a metric affecting roughly 5% to 9% of post-prostatectomy patients—expert advice shifts toward the AUS. This is a clever piece of engineering hidden entirely inside the body. It consists of an inflatable cuff, a pump in the scrotum, and a pressure-regulating balloon. It mimics your original anatomy with surprising fidelity. Which explains why the "bag" conversation is virtually obsolete in modern urology; we have better ways to restore dignity than external plumbing.
Pre-habilitation as a preventative strike
The best way to ensure the answer to "Do you need a bag if you have your prostate removed?" remains a resounding "no" is to start pelvic floor muscle training (PFMT) before the surgeon even touches the scalpel. Clinical data suggests that men who engage in biofeedback-assisted exercises four weeks prior to surgery regain continence up to 40% faster than those who wait until the catheter is removed. It is about muscle memory. If the muscles are thick and responsive before the trauma of surgery, they "wake up" faster once the prostate is gone. As a result: the period of wearing even a small absorbent pad is drastically shortened.
Frequently Asked Questions
Will I have to wear a collection bag during my daughter's wedding three months after surgery?
Absolutely not, provided your recovery is following the standard clinical trajectory. By the 12-week mark, most men have transitioned from heavy pads to either thin liners or total dryness. Statistics from the Journal of Urology indicate that approximately 75% of men achieve social continence—meaning zero to one safety pad—within 90 days of a nerve-sparing procedure. You can wear a tuxedo without any visible bulges or fears of an external apparatus. The only "bag" at the wedding will be the one holding the gifts.
If my incontinence is severe, is a bag better than pads?
There is a device called a condom catheter, which is an external sheath that rolls over the penis and connects to a leg bag, but it is rarely the first choice. Most urologists view this as a temporary solution for skin protection or very specific travel needs rather than a lifestyle. It carries a higher risk of urinary tract infections compared to using high-quality absorbent garments. Unless your dexterity is severely limited, disposable pull-ups are usually the preferred management tool during the healing phase. But remember, this is a bridge, not a destination.
Can the surgery fail so badly that a permanent urostomy bag is required?
In the context of a standard prostatectomy for cancer, a permanent urostomy is virtually unheard of as a direct complication. A urostomy requires the surgeon to divert the ureters into a piece of the small intestine that opens through the abdominal wall, which is a completely different operation. Even in cases of severe urethral stricture or total sphincter failure, we utilize slings or artificial sphincters to fix the problem internally. The structural integrity of the bladder remains intact. Because of this, the fear of "waking up with a bag" is largely rooted in a misunderstanding of pelvic geography.
The final verdict on post-prostatectomy life
We need to stop scaring men with the specter of the permanent urostomy bag. The reality is that modern surgery is a triumph of anatomic preservation, not a gateway to external hardware. You will deal with a catheter for a week, and you might deal with pads for a few months, but the bag is a temporary ghost in the machine. It is high time we prioritize pelvic rehabilitation over surgical anxiety. My stance is firm: the "bag" is an outdated myth for the prostate cancer survivor. If you are prepared, diligent with your exercises, and patient with your biology, your future is dry, internal, and bag-free. In short: keep your dignity and lose the fear.