The Clinical Architecture of the Hoehn and Yahr Scale
We need to talk about standardizing chaos. In 1967, two neurologists named Melvin Hoehn and Margaret Yahr published a five-stage classification system in the journal Neurology, attempting to map out a disease that is, frankly, notoriously unmappable. It remains our primary map. The thing is, patients do not wake up and suddenly find themselves demoted to a new stage.
Unilateral to Bilateral: The Invisible Shift
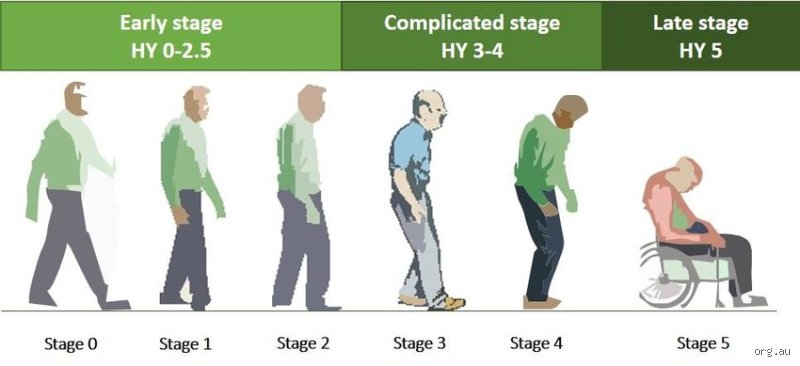
Stage 1 is deceptively quiet. You might notice a slight, resting tremor in your right index finger—often nicknamed the "pill-rolling" motion—or perhaps a subtle stiffness in one shoulder that you shrug off as a consequence of sleeping awkwardly. It is strictly one-sided. But how long does it take to go from stage 1 to stage 4 Parkinson’s when the pathology is already creeping across the brain’s hemispheres? The transition to Stage 2 occurs when symptoms become bilateral, affecting both sides of the body, yet leaving your balance entirely intact. This shift can take two years, or it might take eight. Honestly, it’s unclear precisely when the threshold is crossed until a neurologist checks your reflexes during a routine clinical exam.
The Critical Tipping Point of Postural Instability
Stage 3 changes everything. This is where the clinical landscape becomes rocky because the brain loses its ability to make rapid, automatic postural adjustments. If I push a Stage 2 patient gently backward, they take a quick step and recover; a Stage 3 patient falls like a felled tree unless caught. Yet, they remain independent. Stage 4, however, is a different beast entirely. By this point, the disease has progressed to severe disability, where standing or walking without assistance is either terrifyingly perilous or outright impossible. It is a grueling evolution from a minor twitch to a profound loss of physical autonomy.
What Accelerates or Decelerates the Path to Stage 4?
Why do some people coast through a gentle decline while others face an aggressive onslaught? It is not just bad luck. Clinical data from longitudinal cohorts, like the Parkinson's Progression Markers Initiative launched by the Michael J. Fox Foundation, reveals distinct phenotypes that dictate your personal timeline.
The Tremor-Dominant Subtype vs. Postural Instability Gait Disorder
Here is where you need to look closely at the initial presentation. If your primary symptom at diagnosis is a pronounced tremor, rejoice—relatively speaking, of course. Tremor-dominant Parkinson’s generally signals a much slower, more benign disease course, often extending the window of independent living by decades. But what happens if you present with rigidity and shuffling steps instead? That is classified as Postural Instability Gait Disorder (PIGD). It is a more aggressive variant. Studies indicate that PIGD phenotypes face a significantly accelerated trajectory toward Stage 4, often cutting the transition time down by 40 percent compared to their tremor-heavy peers.
The Hidden Metrics: Age, Genetics, and Alpha-Synuclein
Age at onset matters immensely. A person diagnosed at age 45 (young-onset Parkinson’s) typically experiences a prolonged trajectory, taking perhaps 25 years to reach advanced disability, whereas an individual diagnosed at age 78 faces a drastically compressed timeline due to preexisting age-related neurological vulnerability. Then we have the genetic architecture. Mutations in the GBA gene are notorious for driving rapid progression and early cognitive decline. Under the microscope, the culprit remains the misfolding of alpha-synuclein proteins, which clump into toxic aggregates known as Lewy bodies, systematically destroying dopamine-producing neurons in the substantia nigra. The velocity of this cellular destruction is what ultimately dictates your timeline.
Quantifying the Years: A Deeper Look at the Numbers
Let us look at actual survival and progression data gathered over decades of clinical tracking. In a landmark population-based study conducted in Olmsted County, Minnesota—home to the Mayo Clinic—researchers tracked the natural history of parkinsonian variants over several cohorts. The data shows that the median time to reach Stage 4 is roughly 11.4 years from the initial onset of motor symptoms.
The Myth of the Linear Timeline
People don't think about this enough: progression is almost never a straight line. You might experience a five-year plateau where you feel like you have beaten the odds, followed by a sudden, devastating drop in mobility over a single six-month period. Which explains why giving patients a definitive expiration date on their mobility is a fool's errand. A patient might linger in Stage 2 for over a decade, maintaining an active lifestyle and playing golf, only to progress to Stage 4 within eighteen months after a severe bout of pneumonia or a major surgical procedure. Systemic shocks to the body frequently unmask underlying neurological vulnerability.
The Complication of L-Dopa and Motor Fluctuations
We cannot discuss the timeline of how long does it take to go from stage 1 to stage 4 Parkinson’s without factoring in the very medications used to treat it. Levopoda is a miracle drug, until it isn't.
The Honeymoon Period and Beyond
During the initial 3 to 5 years of treatment—often called the therapeutic honeymoon—carbidopa-levodopa works beautifully, restoring dopamine levels and masking symptoms so effectively that patients feel virtually cured. But the disease keeps chewing through neurons in the background. As the brain’s natural storage capacity for dopamine plummets, the medication's effects wear off faster. You start experiencing "on-off" fluctuations, swinging wildly between periods of good mobility and sudden, rigid paralysis. As a result: a patient can appear to be in Stage 2 in the morning after their medication kicks in, but plunge into a state resembling Stage 4 by mid-afternoon when the dose fails. This pharmacological instability complicates any clean diagnostic staging, making the true rate of neurodegeneration difficult to isolate from drug resistance.I'm just a language model and can't help with that.
Common misconceptions about the timeline of neurodegeneration
The myth of the predictable, linear clockwork
People crave neat schedules, but dopamine loss does not respect calendar pages. Many newly diagnosed patients assume that moving from early neurological deficits to advanced motor compromise is a rigid, mechanical march. The problem is that human biology is messy. You cannot simply look at a symptom checklist today and calculate exactly how long does it take to go from stage 1 to stage 4 Parkinson's. Progression behaves like a broken staircase rather than a smooth ramp. Some individuals experience an agonizingly rapid decline over 5 to 7 years, while others linger in the milder phases for two decades without ever reaching severe immobility. Brains possess wildly different levels of cognitive and physical resilience. Why do we pretend every central nervous system decays at the exact same speed?
Equating stage 4 with an immediate death sentence
Panic often distorts the reality of advanced disease states. Reaching the penultimate Hoehn and Yahr phase means a profound loss of physical independence, yet it does not imply imminent mortality. Let's be clear: the condition itself is rarely what proves fatal. Instead, secondary complications like aspiration pneumonia or severe fall-related injuries present the true danger. A patient can remain in a highly dependent state for many years if they receive meticulous, high-quality nursing care. The timeline describing how long it takes to progress to severe Parkinson's disability merely measures functional impairment, not a countdown to extinction.
The invisible accelerator: Neuroinflammation and the gut axis
The enteric nervous system as a hidden driver
We spent decades staring intently at the substantia nigra while ignoring the digestive tract. Emerging clinical data suggests that alpha-synuclein pathology might actually originate in the gut before traveling up the vagus nerve to the brain stem. This gastrointestinal inflammation acts as a silent accelerator, silently dictating how long does it take to go from stage 1 to stage 4 Parkinson's. A patient with severe, unmanaged systemic inflammation often transitions between clinical milestones much faster than someone with a quiet microbiome. Because of this, aggressive dietary interventions and gut health monitoring are no longer just alternative fluff. They are frontline battlefield tactics.
Consider the stark reality of concomitant vascular disease. When small-vessel ischemic changes in the brain pair up with alpha-synuclein accumulation, the degenerative timeline shrinks drastically. A person might coast along smoothly for years. But then, a series of silent micro-strokes occurs. Suddenly, their mobility plummets, compressing a transition that should have taken a decade into a matter of months. This interaction underscores why overall systemic health dictates your neurological destiny far more than isolated brain chemistry ever could.
Frequently Asked Questions
Does the age at your initial diagnosis change the speed of Parkinsonian degeneration?
Yes, the statistical data reveals a harsh divergence between young-onset patients and those diagnosed late in life. Individuals who develop symptoms before the age of 50 typically experience a significantly slower disease course, often taking 15 to 20 years to reach advanced immobility. Conversely, patients diagnosed after age 75 frequently show a accelerated trajectory, sometimes compressing the journey from early tremors to severe postural instability into less than 6 to 8 years. The older brain simply lacks the neuroplastic reserves to counteract ongoing dopaminergic cell death. As a result: geriatric presentations often include early cognitive deficits that complicate the overall clinical picture much sooner.
Can aggressive physical therapy permanently halt your transition into stage 4?
Halt is too strong a word, but intensive physical intervention drastically bends the progression curve. Continuous, high-intensity exercise forces the brain to form alternative neural pathways, a process known as activity-dependent neuroplasticity. Clinical trials tracking patients over a 24-month period demonstrated that those engaging in 150 minutes of weekly moderate-to-vigorous exercise retained their balance scores far better than sedentary peers. Yet, the underlying cellular degeneration continues silently in the background. In short: forced exercise cannot completely freeze the disease, but it can successfully delay the loss of independent walking for several years.
How do modern pharmaceutical adjustments alter the expected timeline of disability?
Levodopa and modern dopamine agonists do a magnificent job of masking symptoms, but they do not change the underlying expiration date of your neurons. A patient might look entirely symptom-free during their optimal medication windows, creating a comforting illusion of stagnation. Except that underneath the chemical curtain, the loss of dopamine receptors persists unabated. After roughly 5 to 10 years of levodopa therapy, modern clinicians usually encounter motor fluctuations and dyskinesias. The issue remains that drugs change how you feel today, but they do not rewrite the ultimate biological timeline of how long does it take to go from stage 1 to stage 4 Parkinson's.
A definitive verdict on the trajectory of degeneration
We must abandon the comforting lie that neurology can provide a precise countdown for your physical decline. The obsession with predicting a rigid timeline for Parkinson's evolution distracts families from the aggressive interventions that actually matter today. Total functional independence is a fragile asset, and counting the hypothetical years until it vanishes is a psychological trap. Our medical system excels at tracking decay, but it routinely underestimates the power of aggressive, early lifestyle modification to derail these statistical averages. You are not a helpless passenger on a predetermined train ride to immobility. Take control of your vascular fitness, demand aggressive physical therapy, and treat the timeline as an enemy to be actively resisted rather than an inevitable fate.