Understanding Pancreatitis and Why Your Digestive Chemistry Flips Upside Down
The pancreas is a quiet workhorse sitting behind your stomach, producing enzymes like lipase, protease, and amylase. In a healthy body, these enzymes stay dormant until they hit the small intestine. But when pancreatitis strikes, whether it is the sudden lightning bolt of an acute attack or the slow burn of chronic degradation, these chemicals activate prematurely. They literally begin to digest the organ itself. The thing is, your pancreas becomes a biological ticking time bomb where even minor metabolic stress can cause a massive systemic inflammatory response.
The Acute Versus Chronic Divide: Why Timing Alters Your Strategy
Acute pancreatitis hits like a freight train, frequently landing patients in emergency rooms at places like the Mayo Clinic in Rochester or Johns Hopkins Hospital. It demands absolute pancreatic rest, which often means nothing by mouth for days. Chronic pancreatitis, however, is a slow, scarring process that permanently alters your tissue structure over years. And that changes everything because a food that might cause a mild ache in a chronic patient could trigger a life-threatening relapse in someone recovering from an acute episode. Honestly, it is unclear exactly where the threshold lies for every individual, as genetic variances mean one person might tolerate a specific ingredient while another faces immediate hospitalization.
The Diagnostic Markers You Must Monitor Constantly
You cannot manage what you do not measure, which explains why regular lab work is your baseline defense. Doctors look for serum lipase and amylase levels rising three times above the upper limit of normal during an acute flare. For chronic sufferers, monitoring fecal elastase levels becomes paramount to track pancreatic exocrine insufficiency, a condition where the organ stops producing enough enzymes to break down basic nutrients. If your elastase drops below 150 micrograms per gram of stool, your digestive capacity is severely compromised, meaning your tolerance for dietary mishaps drops to virtually zero.
The Hazardous Pharmacy: Medications and Supplements to Cross Off Your List
We often think of food as the primary enemy, but what you swallow from the medicine cabinet can be equally hazardous. Drug-induced pancreatitis accounts for roughly 2% to 5% of all acute cases worldwide, yet people don't think about this enough when grabbing over-the-counter remedies or accepting prescriptions. Your liver isn't the only organ that filters the chemical fallout of modern pharmacology. The pancreas often bears the brunt of cellular toxicity from specific drug metabolites.
Over-the-Counter Hazards: The Hidden Risks of NSAIDs and Acetaminophen
When pain strikes, your first instinct is probably to grab ibuprofen or naproxen. But where it gets tricky is that certain non-steroidal anti-inflammatory drugs have been linked to idiopathic pancreatic inflammation. While infrequent, the risk multiplies dramatically if your organ is already compromised. Acetaminophen overdose is another hidden villain because it depletes glutathione levels, leaving the pancreas vulnerable to oxidative stress. Except that when you are in pain, you need relief; hence, you must consult a gastroenterologist rather than self-medicating with standard drugstore painkillers.
Prescription Culprits: Blood Pressure Meds and Immunosuppressants
Take a close look at your prescription bottles right now. Thiazide diuretics, frequently prescribed for hypertension, are notorious for altering fluid balance and inducing hypercalcemia, which can directly trigger pancreatic enzyme activation. Azathioprine, an immunosuppressant used in autoimmune diseases, carries a documented 5% risk of inducing acute pancreatic inflammation within the first few weeks of therapy. If you are taking these, you cannot simply stop cold turkey, but you absolutely must discuss alternatives with your physician to prevent a pharmaceutical collision course.
The Supplement Trap: Why Natural Is Not Always Safe
The wellness industry loves to push herbal remedies, yet some of these natural extracts behave like chemical weapons inside an inflamed GI tract. High-dose vitamin C supplements can alter metabolic pathways, while concentrated green tea extracts have occasionally shown direct organ toxicity. Most dangerous, however, are unregulated herbal blends containing high levels of calcium or iron. Excess calcium in the bloodstream acts as a fuse for trypsinogen activation inside the pancreatic acinar cells, transforming a helpful supplement into an internal matchstick.
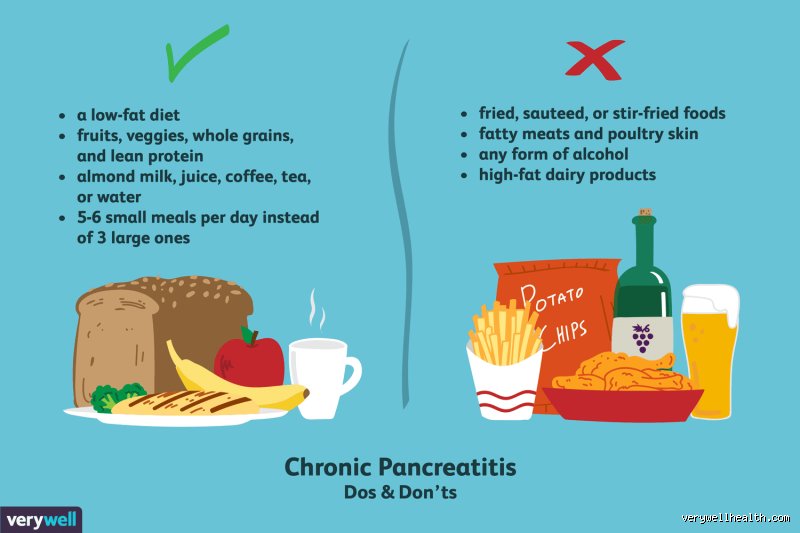
Dietary Landmines: The Specific Nutrients That Trigger Enzyme Chaos
Food is the most frequent trigger for the intense pain associated with this condition. When you swallow fat, your duodenum secretes cholecystokinin, a hormone that commands the pancreas to pump out digestive fluids. If the organ is inflamed, this hormonal command is the equivalent of whipping a exhausted horse. You need to know exactly which molecular structures cause this backlash.
The Myth of Healthy Fats: Why Avocado and Olive Oil Can Still Harm You
Conventional nutritional wisdom says that extra virgin olive oil and avocados are dietary heroes because they contain monounsaturated fatty acids. But your pancreas does not care about the origin of the lipid molecule; it only cares about the total mass it has to break down. I must take a sharp stance here: during the recovery phase, a gram of fat from an organic avocado puts the exact same workload on your pancreas as a gram of fat from a commercial fast-food burger. While the long-term nutritional profile differs, the immediate mechanical stress on your digestive tract remains identical, meaning even these healthy fats must be restricted to less than 30 to 50 grams per day depending on your specific tolerance level.
Processed Carbohydrates and High-Fructose Corn Syrup: The Insulin Spike Danger
People focus so intensely on fat that they completely overlook the carbohydrate danger. Refined sugars, white bread, and pastries cause rapid spikes in blood glucose, forcing the endocrine portion of the pancreas to pump out massive amounts of insulin. Because the organ is already inflamed, this metabolic demand worsens local tissue stress. Furthermore, diets rich in high-fructose corn syrup rapidly elevate blood triglyceride levels, which is a direct, independent mechanism for triggering acute attacks.
Evaluating Fat Substitutes and Medium-Chain Triglycerides against Standard Dietary Lipids
When standard fats are off the table, patients often look for loopholes to maintain their caloric intake and keep food tasting palatable. This search brings us to the debate surrounding different lipid structures and how the human body processes them under metabolic duress. It is a territory where nuance is required because what works in a laboratory setting doesn't always translate perfectly to the human dinner plate.
The Structural Difference: Long-Chain vs. Medium-Chain Fatty Acids
Standard dietary fats consist of long-chain triglycerides that require pancreatic lipase and bile salts for emulsification and absorption. Medium-chain triglycerides, or MCTs, are processed differently by the body. They bypass the standard pancreatic digestion pathway, absorbing directly into the portal vein via the liver. This unique pathway makes MCT oil a valuable tool for maintaining caloric density without forcing the pancreas to work overtime. However, experts disagree on the dosage, because consuming too much MCT oil too quickly can lead to severe abdominal cramping and osmotic diarrhea, mimicking the very symptoms you are trying to avoid.
The Real-World Comparison: Coconut Oil Versus Pure MCT Formulations
Many patients mistakenly substitute commercial coconut oil for pure MCT oil, believing them to be identical. This is a critical mistake. Coconut oil contains only about 55% true medium-chain fatty acids, with the remainder composed of lauric acid and other long-chain lipids that still require pancreatic lipase for breakdown. Pure, medical-grade MCT oil is 100% caprylic and capric acid. In short, using standard coconut oil as a cooking substitute during a pancreatitis recovery phase can inadvertently overload your digestive system with the exact long-chain fats your doctor told you to avoid.