The Anatomy of Coitus Interruptus and Why We Still Depend on It
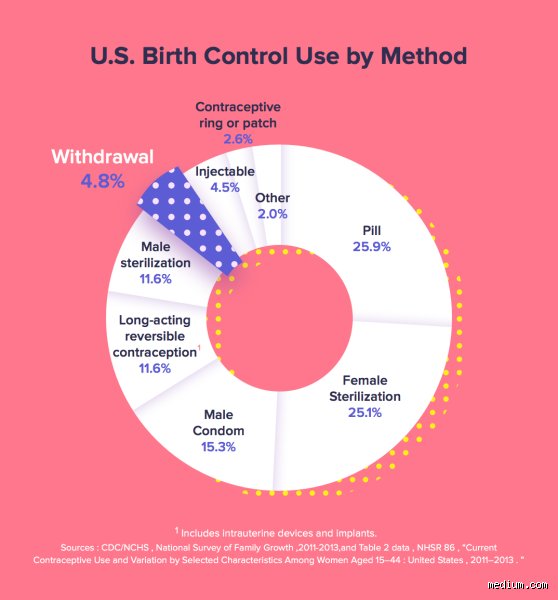
We need to talk about why an ancient contraceptive strategy—historically known as coitus interruptus—remains stubbornly popular in an era of subcutaneous implants and high-tech hormonal rings. The thing is, modern medicine loves to dismiss it with a patronizing chuckle, yet global health data tells a completely different story. In 2002, the Centers for Disease Control and Prevention (CDC) in Atlanta noted that over half of American women had relied on withdrawal at some point in their reproductive lives. Why? Because it costs exactly zero dollars, requires no pharmacy trips, and is instantly reversible. But where it gets tricky is defining what "doing it right" actually means in the heat of the moment.
The Mechanics of Perfect vs. Typical Control
Perfect use is a clinical fantasy. To achieve that 4% perfect-use failure rate, the penetrating partner must possess an almost superhuman level of self-control, accurately predicting the exact moment of ejaculation and withdrawing the penis completely away from the vulva before a single drop of semen escapes. But human beings are not Swiss watches. Typical use—which factors in late withdrawals, midnight miscalculations, and alcohol-blurred judgment—drastically alters the math. When you realize that nearly a quarter of typical users end up pregnant within twelve months, the conventional medical wisdom that labels this method a total disaster starts to make sense, yet millions continue to use it successfully for decades. Honestly, it's unclear why some couples seem completely immune to its risks while others fail immediately.
The Hidden Biological Minefields: Pre-cum, Sperm Motility, and Secretion
People don't think about this enough: the real danger isn't always the obvious tidal wave of semen at the end, but the mysterious fluid that comes before it. This fluid, secreted by the Cowper’s glands during arousal, acts as a natural lubricant and acid neutralizer. By itself, pure pre-ejaculatory fluid does not contain sperm. Yet, a landmark 2011 study conducted by researchers at the Contentious Issues in Sexual Health clinic in the UK threw a massive wrench into this comforting assumption. They found viable, moving spermatozoa swimming around in the pre-cum of 41% of their male subjects. That changes everything.
Where did those rogue swimmers come from? They were the leftovers. If a man has ejaculated recently—say, earlier that morning—viable sperm can linger inside the urethral tract like unwanted guests after a party. The next time he gets aroused, the Cowper's fluid flushes through the urethra, inadvertently loading the chambers with residual ammunition. I find it fascinating that human anatomy has this built-in design flaw, a biological booby trap that turns a moment of high friction into an accidental conception event. Unless the partner urinates between sessions to clear the pipes, the effectiveness of the strategy plummets before the act even begins.
The Secret Role of Vulvar Ingress
Here is another uncomfortable truth that sex education classes usually gloss over: you do not need full penetration to cause a pregnancy. If withdrawal happens a fraction of a second too late, and semen lands directly on the labia majora or near the vaginal opening, the biological machinery takes over. Sperm cells are microscopic, chemically driven survivalists equipped with flagella designed for one specific purpose: swimming toward cervical mucus. Ambient moisture on the vulva can act as a temporary highway. Because of this, pulling out and ejaculating on the external genitalia is barely safer than not pulling out at all, which explains why so many frantic calls are made to pharmacies regarding emergency contraception the morning after.
Quantifying the Risk: What the Contraceptive Data Actually Reveals
To understand the true landscape of how effective is the pull-out method, we have to stack it directly against the gold standards of birth control. The Princeton University contraceptive metrics provide an excellent, albeit sobering, reality check. When you look at long-acting reversible contraceptives (LARCs) like the Mirena intrauterine device or the Nexplanon arm implant, the failure rates hover around a microscopic 0.05% to 0.2%. Those are systems designed to remove human fallibility entirely from the equation. The comparison looks bleak, as a 22% typical-use failure rate means withdrawal is roughly as effective as using male condoms poorly, but significantly worse than the birth control pill.
But let us look at the data from an inverse perspective to find some nuance. A 78% success rate under typical conditions means that for a huge portion of the population, the method actually works out in their favor over short durations. It is a statistics game. If a couple in Chicago uses withdrawal exclusively for a single month, their risk of pregnancy is relatively low; however, cumulative risk is a patient predator. Over five years of continuous exposure to that annual 22% roll of the dice, the probability of an unintended pregnancy climbs exponentially, converting a casual habit into a statistical certainty.
The Asymmetry of Pleasure, Risk, and Relationship Dynamics
We cannot analyze the question of how effective is the pull-out method without examining the psychological friction it introduces into a relationship. The burden of execution falls entirely on one partner, while the physical consequences of failure are borne almost exclusively by the other. This creates a bizarre, tense interpersonal dynamic. The penetrating partner must remain hyper-vigilant, monitoring their internal neurological triggers right when their brain is screaming for them to do the exact opposite. It requires pulling away at the peak of physical pleasure, an act that fundamentally contradicts basic human wiring.
The Anxiety Coefficient of Unprotected Sex
What about the mental toll? Sex is supposed to reduce cortisol, yet relying on withdrawal often turns intimacy into a high-anxiety performance review. You are constantly questioning the timing: Did he get out fast enough? Was that wetness just lubrication or something else? This chronic background worry can erode sexual satisfaction over time, acting as a psychological contraceptive by making the act itself too stressful to enjoy. As a result: couples often cycle between periods of strict withdrawal use and panicked runs to buy Plan B, living in a constant state of low-grade reproductive panic that no medical textbook can truly quantify.
Common mistakes and dangerous assumptions
The "just-in-time" delusion
Timing is everything, yet human panic destroys precision. Many couples believe intuition dictates the exact millisecond before ejaculation occurs, but biological reality laughs at this confidence. The friction of intercourse dulls sensory awareness. As a result: the male partner often retreats a fraction of a second too late, leaving the initial, highest-concentration wave of spermatozoa right at the cervix. This fluid contains the highest sperm count. A single millimeter of delay defeats the entire purpose of the pull-out method.
The toxic myth of the second round
You cannot simply wipe the surface and resume immediately. Residual semen lurks inside the urethra after the first climax. When excitement returns, the subsequent pre-ejaculatory fluid flushes these dormant, highly viable cells directly into the partner. Because people forget basic plumbing, unexpected pregnancies spike during weekend marathons. Urinating between sessions helps clear the tract, except that it provides no absolute guarantee. Coitus interruptus failure rates skyroment when alcohol or fatigue blurs judgment during consecutive rounds.
Ignoring the anatomical spillover
Withdrawing means clearing the entire vicinity, not just exiting the vaginal canal. Depositing semen directly onto the vulva or external labia still creates a highly perilous pathway for motile cells. Fluids migrate easily. Can we really trust liquid to stay exactly where it lands during frantic movement? Liquid flows, and sperm swim upward through wet environments, meaning external ejaculation often equals internal exposure.
The hidden biochemistry of pre-ejaculate
The great pre-cum debate solved by science
Medical textbooks historically claimed that pure pre-ejaculatory fluid from the Cowper's gland contains zero sperm. That remains technically true in a sterile vacuum, yet real-world testing tells a far more volatile story. Recent laboratory insights show that up to 41 percent of men harbor active, motile spermatozoa in their pre-cum even without prior recent ejaculations. The problem is that you cannot predict which category your partner falls into without a microscope. Some individuals are constant leakers of mobile sperm, which explains why the withdrawal technique effectiveness plummets even when execution seems flawless. (Talk about an awkward genetic lottery.) It turns out that tracking ovulation becomes your only real shield if you insist on playing this specific roulette.
Frequently Asked Questions
Can you get pregnant from pre-cum using the pull-out method?
Yes, the risk is statistically significant and clinically proven. A landmark study published in Human Fertility examined fluid samples and discovered viable sperm in over 40 percent of male subjects before ejaculation. These cells were not just present; they were highly motile and fully capable of fertilization. The perfect-use failure rate sits at 4 percent annually, but this biological variable pushes typical real-world failure up to a staggering 20 percent. You are gambling on whether a specific partner leaks active cells during arousal.
Does pulling out offer any protection against STIs?
Absolutely not, because pathogens do not wait for the grand finale. Infections like chlamydia, gonorrhea, and human papillomavirus thrive in the mucosal membranes and are transmitted through simple skin-to-skin contact or pre-ejaculatory secretions. Furthermore, HIV viral loads in pre-cum are high enough to transmit the virus without full ejaculation. In short, using the pull-out method as infection control is entirely useless. Only physical barriers block microscopic pathogens effectively.
How does the efficacy of withdrawal compare to emergency contraception?
If your timing fails, relying on the morning-after pill alters your statistical safety net entirely. Standard levonorgestrel emergency pills reduce the risk of pregnancy by roughly 85 percent if taken within 72 hours of the mishap. However, these rescue medications lose efficacy drastically if your weight exceeds 165 pounds or if ovulation has already occurred. The natural family planning alternative becomes a chaotic guessing game once semen makes contact. Combining withdrawal with immediate emergency intervention is the only way to salvage a late exit.
A definitive verdict on withdrawal
Let's be clear: relying on withdrawal as your primary shield is akin to driving a car without an airbag because you trust your reflexes. The math does not lie, and a twenty percent annual failure rate means one in five couples will face an unplanned pregnancy within twelve months. We must stop treating this anatomical gamble like a legitimate medical strategy when affordable, highly effective barriers and hormonal options exist. It functions passably as an emergency backup or a secondary layer when combined with fertility awareness tracking, yet on its own, it demands perfection from an imperfect human act. Your reproductive autonomy deserves far better than a strategy built entirely on frantic timing and biological luck. Take control of your future rather than leaving it to a split-second physical reflex.