The Hidden Battlefield: Anatomy of the Intestinal Tract Under Siege
To truly comprehend which organ is affected by diarrhea, we must look past the stomach. The human gut is a six-meter pipe of sheer complexity. Food enters the small intestine—comprising the duodenum, jejunum, and ileum—where the vast majority of nutrient extraction happens. But water is the real currency here. Every single day, your digestive system processes roughly 9 liters of fluid, including saliva, gastric juices, and bile. Yet, you only excrete about 100 to 200 milliliters in normal stool. Where does the rest go?
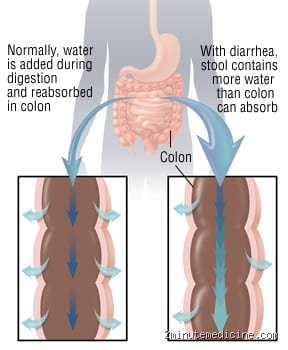
The Colon as the Master Sponge
Enter the large intestine. If the small intestine is the chaotic processing plant, the colon is the pragmatic recycling facility. It absorbs the remaining water and electrolytes, transforming liquid chyme into solid waste. When pathogens like Campylobacter jejuni or rotavirus invade, this exquisite sponge mechanism fails completely. The mucosal lining becomes inflamed, and instead of pulling water out of the waste, the cells start pumping fluid into the lumen. That changes everything. The colon suddenly shifts from an absorbent organ to a hyper-secreting faucet, resulting in the loose, watery stools we all dread.
When Peristalsis Goes into Overdrive
The issue remains that absorption is only half the battle. Your gut relies on peristalsis, a rhythmic wave of muscular contractions that pushes contents forward at a leisurely pace. But during an infection, the enteric nervous system panics. It triggers a frantic clearance mechanism, which explains the agonizing cramps that precede an emergency bathroom run. Honestly, it's unclear whether the body does this to protect itself or if the bacteria are hijacking our plumbing for their own evolutionary gain, but the result is a massive acceleration of transit time.
Technical Breakdown: The Molecular Sabotage of the Small Intestine
We need to talk about the small intestine because people don't think about this enough. While the colon determines the final consistency of your stool, the small intestine is often where the initial biochemical sabotage occurs. Think of the microscopic villi—tiny, finger-like projections—as a vast landscape. During a severe bout of diarrhea, this landscape is utterly flattened. In a famous 2018 study conducted at Johns Hopkins University, researchers demonstrated how specific strains of enterotoxigenic Escherichia coli (ETEC) release toxins that disrupt the intracellular cyclic AMP levels in these villi.
The Sodium-Glucose Cotransporter Breakdown
This is where it gets tricky. Normally, your gut cells use a mechanism called the Sodium-Glucose Cotransporter 1 (SGLT1) to drag nutrients into the bloodstream. Water passively follows these solutes. But when bacterial toxins block this channel, sodium remains trapped in the intestinal lumen. Because of basic osmosis, water refuses to cross the cellular membrane. It stays in the pipe. You can drink gallons of pure water during a cholera outbreak, but without the correct balance of glucose and sodium, it will pass straight through you, exacerbating the dehydration. This fundamental flaw in cellular mechanics is why diarrheal diseases remain the second leading cause of death in children under five globally, accounting for roughly 525,000 child fatalities annually according to the World Health Organization.
Secretory Versus Osmotic Chaos
Not all diarrheas are created equal, mind you. Clinicians divide the pathology into distinct categories based on which cellular mechanism is misbehaving. Secretory diarrhea, often triggered by the cholera toxin, forces crypt cells to actively secrete chloride ions into the gut. Osmotic diarrhea, conversely, happens when you ingest something unabsorbable—like excessive sorbitol in sugar-free gum or lactose in someone who lacks lactase. The unabsorbed molecules act like a chemical magnet, pulling water out of the body's tissues and into the bowel. The distinction matters immensely for treatment, yet the victim on the toilet rarely cares about molecular polarity while fighting for survival.
The Colonic Disruption: How the Large Intestine Loses Control
Let us move down to the large intestine, a tract roughly 1.5 meters long that houses trillions of microbes. When looking at which organ is affected by diarrhea from a chronic perspective, the colon takes center stage. Diseases like Ulcerative Colitis or Crohn's disease don't just cause temporary fluid shifts; they structurally alter the colonic architecture. The mucosal barrier, which should be an impenetrable fortress, develops deep, bleeding ulcers.
The Loss of Short-Chain Fatty Acids
Here lies a fascinating paradox that experts disagree on. Your colonocytes—the cells lining the large intestine—derive up to 70% of their energy not from the bloodstream, but from short-chain fatty acids (SCFAs) like butyrate, which are produced by your gut bacteria fermenting dietary fiber. When diarrhea flushes out the microbiome, the colonocytes are effectively starved. They lose their structural integrity. Without their energy source, these cells cannot maintain the tight junctions that prevent fluid leaks, creating a vicious cycle where the diarrhea itself perpetuates further tissue damage.
Comparing Intestinal Failure: Small Bowel vs. Large Bowel Pathologies
How do we distinguish which organ is affected by diarrhea based on symptoms alone? It turns out the stool tells a vivid anatomical story. When the pathology resides primarily in the small intestine, the resulting diarrhea is typically voluminous, watery, and less frequent. You might only go to the bathroom three times a day, but the sheer output is staggering because the major absorption zone has gone offline. Think of it like a broken dam at the top of a river valley.
The Distal Disturbance
But when the colon is the primary site of injury—as seen in Shigellosis outbreaks or amoebic dysentery—the clinical presentation flips completely. The stools are small, frequent, and often laced with blood, mucus, and inflammatory cells. Doctors call this phenomenon tenesmus, a distressing, painful sensation where you feel the constant urge to evacuate even though the colon is practically empty. The nerves in the rectal wall are so inflamed that they constantly misfire, sending false alarms to the brain. We are far from a simple plumbing issue here; it is a profound neurological and immunological breakdown at the tail end of the digestive tract.
Common mistakes and misconceptions about intestinal distress
The stomach is not the culprit
People constantly blame their stomach when their digestive system goes rogue. They point at their upper abdomen and groan about a bug. Let's be clear: your stomach is almost never the answer to which organ is affected by diarrhea. That acidic pouch merely liquefies food before sending it downstream. The real battleground lies much lower, specifically within the twisted loops of your small intestine and the colon. Why do we misidentify the location? Because visceral pain is notoriously vague, tricking your brain into thinking the upper gastric zone is suffering when the lower bowel is actually flooding its banks.
Imodium is not a universal cure
You feel a rumble and instantly reach for anti-motility drugs. Stop right there. Halting the muscular contractions of your colon can sometimes backfire spectacularly. If a hostile strain of *Salmonella* or *Shigella* is throwing a party in your gut, your body uses loose stools as a biological eviction notice. Forcing the plumbing to shut down keeps those pathogens trapped inside the lumen. The problem is that paralyzed intestines give bacteria more time to breach the epithelial barrier, potentially worsening your condition. Except that sometimes you do need a break from the bathroom, but blind self-medication is a gamble.
The enteric nervous system: The hidden driver of bowel dysfunction
Your second brain is pulling the strings
Did you know your gut houses over 100 million neurons? This dense mesh of nervous tissue is the enteric nervous system, and it governs the exact way organs impacted by watery stool behave. When you experience severe stress, your brain floods your system with cortisol and adrenaline. The issue remains that your gut mimics this panic. This neural network can instantly trigger hypermotility, forcing the colon to contract violently and dump its contents before proper water absorption can happen.
[Image of the enteric nervous system]Microscopic inflammation changes everything
Sometimes, the tissue looks completely normal under a standard colonoscopy. Yet, on a cellular level, a war is raging. Tiny tight junctions between your intestinal cells act like standard cellular mortar. When these junctions fail due to low-grade inflammation, water leaks freely into the intestinal lumen instead of being absorbed. Which explains why some people suffer from chronic, unexplained loose bowel movements despite flawless medical scans.
Frequently Asked Questions
Can a damaged small intestine cause acute diarrhea?
Absolutely, because the small intestine is responsible for absorbing roughly 90% of the fluids you ingest daily. When pathogens like *Rotavirus* destroy the microscopic villi lining this tube, the surface area available for fluid uptake drops by up to 60 percent. As a result: unabsorbed water and solutes rush straight into the large bowel, completely overwhelming its capacity. This specific mechanism results in massive, high-volume watery stools that can dehydrate a teenager or an adult within mere hours if left unchecked.
How long does the colonic lining take to heal after an infection?
The human intestinal epithelium is one of the fastest-regenerating tissues in the entire body, typically replacing its entire cell surface every three to five days. However, a severe bout of *Campylobacter* or *Giardia* can leave behind microscopic raw patches that persist for weeks. (This lingering irritation is often diagnosed as post-infectious irritable bowel syndrome). Statistics show that up to 10% of individuals who experience acute bacterial gastroenteritis will suffer from altered bowel habits for months afterward, even though the original pathogen is long gone.
Does routine antibiotic use permanently alter which organ is affected by diarrhea?
Antibiotics don't just target the bad bacteria; they obliterate your protective microbiome, directly shifting how the large intestine functions. A single course of broad-spectrum antibiotics can disrupt your gut ecosystem for up to 180 days, reducing microbial diversity by nearly a third. Without these beneficial microbes to ferment dietary fiber into short-chain fatty acids, the colon loses its primary energy source. Consequently, the colon mucosal barrier weakens, making the large intestine uniquely vulnerable to opportunistic infections like *Clostridioides difficile*.
A final verdict on the gut battleground
We need to stop viewing loose stools as a simple, isolated inconvenience and recognize it as a profound systemic failure of intestinal transport. The medical community often focuses heavily on the colon, but the entire gastrointestinal tract operates as a single, delicate domino line. If your small intestine fails to absorb nutrients, your large intestine will inevitably bear the brunt of the fluid overload. It is high time we abandon outdated home remedies and respect the intricate neural and cellular architecture governing our digestive health. Your gut isn't just misbehaving; it is actively fighting a microscopic war to protect your entire body from toxic invaders.