Decoding the Diagnostic Tangle: Is Autism Itself a Psychiatric Condition?
Let us clear the air immediately because a massive amount of confusion lingers in mainstream medical discourse. Autism spectrum disorder (ASD) sits firmly in the neurodevelopmental category of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), meaning it originates during early brain development. It changes how a person processes sensory information, navigates social communication, and perceives the world. Psychiatric comorbidities develop alongside autism, triggered by a mix of biological vulnerabilities and the sheer, exhausting friction of navigating a world built for neurotypical brains. The thing is, clinicians spent decades misdiagnosing autistic adults—especially women and non-binary individuals—with personality disorders before realizing the underlying architecture was neurodivergence all along.
The Shadow of Misdiagnosis in Psychiatric History
Go back to London in the late 1990s, where clinical practices routinely mislabeled autistic women as having Borderline Personality Disorder (BPD). Why? Because the intense emotional dysregulation and social masking looked identical from the outside to an untrained examiner. But here is where it gets tricky: a meltdown caused by sensory overload at a train station is fundamentally different from a BPD emotional crisis rooted in a fear of abandonment. We are far from a perfect diagnostic system, and historically, thousands of people spent years taking the wrong medications because psychiatrists failed to see the autistic traits underneath the anxiety. The issue remains that our diagnostic tools were validated almost exclusively on young boys, leaving everyone else vulnerable to slipping through the psychiatric cracks.
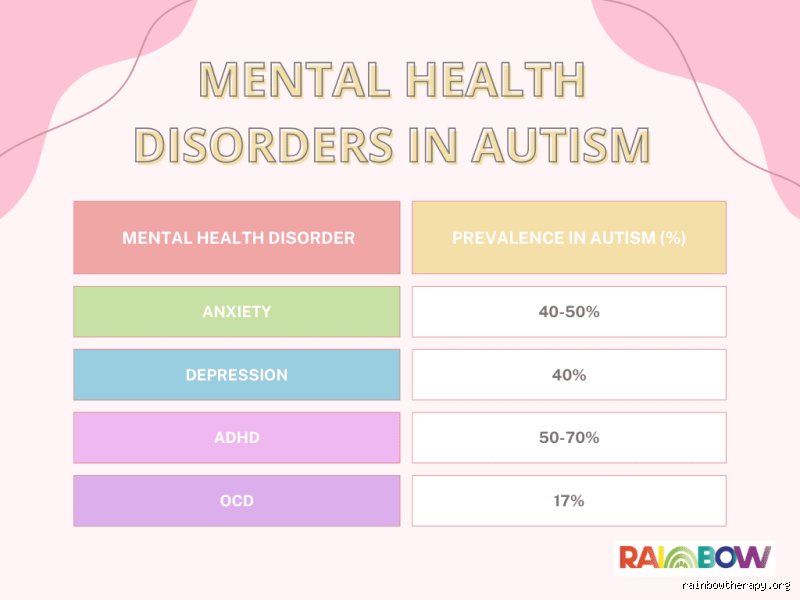
The Heavyweight Contenders: Anxiety and Depression on the Spectrum
When exploring what mental illness is associated with autism, generalized anxiety disorder and major depressive disorder emerge as the most prevalent tormentors. This is not just a statistical quirk; it is a lived reality for nearly half the spectrum. Think about the cognitive load required to manually calculate every blink, nod, and conversational turn during a standard job interview. That constant state of hyper-vigilance inevitably cooks the nervous system, turning situational stress into a chronic, clinical anxiety state. Yet, mainstream clinics often treat this as standard anxiety, ignoring the fact that traditional exposure therapy can actually traumatize an autistic person if the trigger is a genuine, agonizing sensory intolerance to fluorescent lights or loud noises.
The Constant Burnout Leading to Depressive Regression
Imagine living in a world where your natural state of being is considered a deficit that needs fixing. That changes everything, doesn't it? This relentless pressure to conform leads directly to autistic burnout, a state of profound physical and mental exhaustion that looks exactly like severe clinical depression but behaves very differently. A landmark 2015 study by researchers in Sweden tracked over 27,000 autistic individuals and found they were more than ten times as likely to die by suicide than the general population. It is a staggering, heartbreaking statistic. Because traditional talk therapy relies heavily on identifying vague emotional states, it often fails miserably for autistic individuals who experience alexithymia—the inability to identify or describe one's own emotions.
The Sensory Overload Connection to Panic Disorders
People don't think about this enough, but our physical environment is a sensory minefield. A crowded supermarket in downtown Chicago or a bustling school cafeteria in London can easily trigger a full-scale panic attack. Except that it might actually be a sensory meltdown masquerading as panic. Which explains why standard anti-anxiety interventions frequently bomb in neurodivergent populations; you cannot cognitively reframe a neurological intolerance to high-frequency sounds. As a result: we see individuals withdrawing completely from society, an isolated existence that then feeds directly back into the depressive cycle.
The Complicated Intersection of ADHD and Obsessive-Compulsive Tendencies
For a long time, the DSM strictly forbade diagnosing someone with both autism and Attention-Deficit/Hyperactivity Disorder (ADHD). It was an absurd, bureaucratic rule that ignored the bleeding obvious. In 2013, the medical establishment finally relented, and today we know that roughly 50% to 70% of individuals with autism also present with significant ADHD symptoms. This combination creates a chaotic internal paradox: the autistic brain craves rigid structure, predictability, and deep focus, while the ADHD brain demands novelty, dopamine, and constant stimulation.
When Rituals Cross the Line Into OCD
Where does a passionate autistic special interest end and Obsessive-Compulsive Disorder (OCD) begin? Experts disagree on the exact boundary, and honestly, it's unclear in many clinical presentations. An autistic individual might arrange their books by publication date because it brings them deep comfort and neurological calm. But if they are rearranging those books because they believe their family will perish in a terrible accident if they don't, that is clinical OCD. Distinguishing between distress-driven compulsions and comfort-driven repetitive behaviors is the pivot point for effective treatment, yet many therapists still muddle the two.
Differential Realities: Traumatic Stress Versus Neurodevelopmental Traits
We absolutely must talk about Complex Post-Traumatic Stress Disorder (C-PTSD). Growing up autistic in a neurotypical society is, by its very definition, a series of micro-traumas. Chronic bullying, social rejection, and being forced to suppress natural self-regulatory behaviors (like hand-flapping or rocking) leaves a lasting scar on the psyche. But wait, is it actually a distinct mental illness, or is it just the inevitable consequence of systemic lack of accommodation? Many modern clinicians argue that much of the anxiety we associate with autism is actually untreated trauma from trying to survive in a hostile environment.
The Bipolar Overlap and Schizophrenia Myths
Historically, early 20th-century psychiatry actually classified autism as a childhood form of schizophrenia. We now know they are entirely distinct, though they share some genetic vulnerabilities. Bipolar disorder also shows up at higher rates on the spectrum, particularly Bipolar II, where hypomanic episodes can easily be mistaken for an autistic individual's intense, high-energy hyper-fixation on a new project. Hence, the diagnostic waters remain muddy, requiring a level of clinical nuance that standard fifteen-minute psychiatric evaluations simply cannot provide. The article continues below.
Common diagnostic traps and weaponized misconceptions
The diagnostic overshadowing eclipse
Psychiatrists frequently look at an autistic individual through a distorted lens. They spot the blatant sensory meltdowns or the intense, hyper-focused interests and instantly attribute every single psychological tremor to the developmental condition itself. This clinical blind spot is known as diagnostic overshadowing. Except that generalized anxiety or major depressive disorder do not simply vanish just because someone possesses an atypical neurotype. The problem is that treatable internalizing disorders get ignored while clinicians chalk up profound lethargy or panic attacks to standard autistic burnout. Why do we keep separating the mind into neat, isolated filing cabinets when biology clearly prefers messy, overlapping networks?
The trauma-masking conflation
Camouflaging autistic traits to survive in a neurotypical world requires immense cognitive effort. This chronic masking often mimics or directly triggers complex post-traumatic stress disorder, blurring the lines of what mental illness is associated with autism during standard psychiatric evaluations. The constant hypervigilance looks identical to borderline personality disorder or paranoid ideation. Let's be clear: forced behavioral conformity is a reliable engine for psychological trauma. When a clinician misinterprets this deeply ingrained survival strategy as an inherent personality defect, the subsequent treatment plan inevitably fails because it targets the armor rather than the wound.
The sensory-emotional bottleneck and expert intervention
Interoceptive blindness as a psychiatric amplifier
Many autistic adults live with poor interoception, the internal sensory system that tells us whether our heart is racing from fear, excitement, or merely an extra cup of espresso. This creates a terrifying emotional bottleneck. An individual might experience a massive spike in physiological arousal without any cognitive awareness of the trigger until a full-blown panic episode manifests. But traditional cognitive behavioral therapy relies heavily on recognizing early emotional shifts. As a result: standard therapeutic modalities must be radically dismantled and rebuilt for neurodivergent anatomy. Experts now advocate for somatic-based interoceptive retraining before any traditional talk therapy is introduced. If you cannot accurately map your own heartbeat, trying to restructure your cognitive distortions is an exercise in futility.
Frequently Asked Questions
Is ADHD considered a comorbid mental illness associated with autism?
Attention-deficit/hyperactivity disorder is classified as a neurodevelopmental condition rather than a psychiatric illness, yet its co-occurrence rate with autism is astonishingly high. Genomic data indicates that approximately 50% to 70% of autistic individuals exhibit significant ADHD symptoms simultaneously. This overlapping presentation complicates the diagnostic landscape significantly, frequently delaying accurate support until adulthood. The issue remains that clinicians historically viewed these two profiles as mutually exclusive categories according to older diagnostic manuals. Modern psychiatric frameworks now recognize that their shared genetic architecture creates a uniquely chaotic executive functioning profile that demands integrated, non-linear therapeutic approaches.
How does the prevalence of depression in autistic individuals compare to the general population?
Epidemiological research reveals a stark, deeply troubling disparity when examining affective disorders within this demographic. Large-scale meta-analyses show that clinical depression affects roughly 32% of autistic adults, a figure that dwarfs the estimated 7% prevalence rate found across neurotypical control groups. This dramatic inflation stems from chronic social isolation, systemic employment discrimination, and the relentless exhaustion of navigating hostile sensory environments. Which explains why clinicians must screen for vegetative depressive symptoms during every routine checkup. We cannot treat this epidemic of low mood as an unavoidable tax for being neurodivergent; it is a direct consequence of a society refusing to build accessible spaces.
Why are eating disorders frequently misdiagnosed in neurodivergent patients?
Anorexia nervosa shares a surprisingly robust, hidden relationship with the autistic phenotype, particularly among females. Recent clinical audits suggest that up to 20% of women presenting with severe restrictive eating behaviors demonstrate significant, previously undiagnosed autistic traits. The underlying motivation in these specific cases rarely centers on Western aesthetic ideals of thinness or body dysmorphia (a common misinterpretation that derails traditional eating disorder recovery programs). Instead, the restriction acts as a profound coping mechanism to manage severe gastrointestinal distress, sensory aversion to specific food textures, or an obsessive need for predictability in a chaotic world. In short, treating the eating behavior without accommodating the sensory profile guarantees a high relapse rate.
A radical realignment of psychiatric priorities
We must stop treating comorbid psychiatric conditions in neurodivergent populations as unexpected, anomalous anomalies. The data screams a different truth: experiencing an Axis I psychiatric condition is the statistical norm, not the exception, for those on the spectrum. Let's stop forcing these complex individuals into rigid, neurotypical therapeutic boxes that only exacerbate their alienation. Our current mental health infrastructure remains fundamentally broken because it views autistic distress as a defect to be cured rather than a systemic mismatch to be accommodated. True clinical progress requires us to fiercely reject behavioral compliance models. We must boldly pioneer an adaptive, neurodiversity-affirming paradigm that prioritizes nervous system safety over superficial social assimilation.