The Global Landscape of the Uncut: Demographics and Definitions
To understand the variance in surgical rates, one must first dismantle the assumption that geography equals ethnicity. It does not. While international health agencies often publish data broken down by nation-state, the underlying driver of whether a man keeps his foreskin is almost always his cultural heritage, religious affiliation, or ethnic lineage. Because of this, mapping the practice requires an anthropological lens. For instance, a person of Han Chinese descent living in San Francisco is statistically far less likely to be circumcised than their neighbor of Caucasian or Jewish descent, despite sharing the exact same zip code and medical system.
Decoupling Medical Directives from Cultural Inheritance
The global distribution of this procedure is a patchwork quilt of ancient taboos and colonial interventions. In Western Europe, the shift away from infant circumcision occurred rapidly after World War II, when national healthcare systems—such as the National Health Service (NHS) in the United Kingdom—concluded that the procedure lacked compelling medical necessity. Consequently, modern ethnic English, French, and Scandinavian populations have become overwhelmingly intact. Yet, if you look at data from the World Health Organization (WHO), the numbers are often aggregated in ways that obscure the reality of minority ethnic enclaves within those very nations. It is a nuanced picture, and honestly, it's unclear why some epidemiological studies still insist on blending these distinct groups into broad, unhelpful regional averages.
The East Asian Paradigm: Why Han Chinese and Japanese Populations Remain Intact
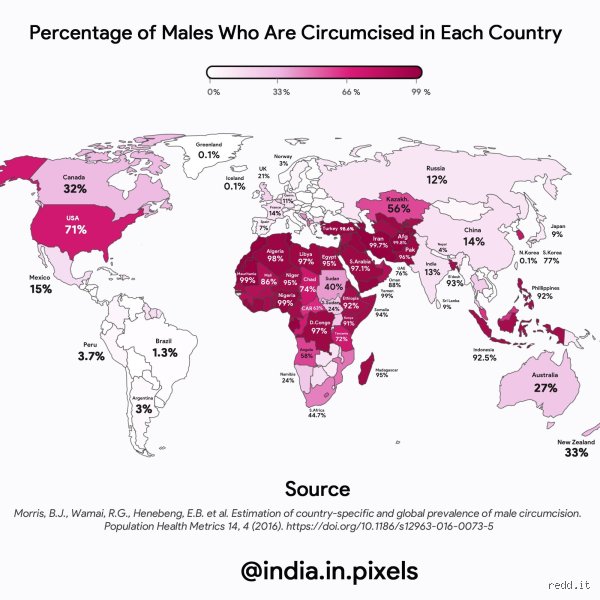
If you want to find the absolute statistical floor for this procedure, you have to look at East Asia. Among the Han Chinese population, which constitutes over 90% of the population of China and numbers greater than 1.3 billion people globally, circumcision is exceedingly rare, hovering consistently around the 0.5% to 1% mark. Why is this? The answer lies in Confucian philosophy. Traditional Chinese culture places an immense spiritual and ethical value on maintaining the integrity of the body given by one's parents. Altering the anatomy without an existential, life-threatening medical crisis is traditionally viewed as a breach of filial piety—a concept that deeply influences even highly secularized, modern Chinese communities today.
The Japanese Deviation and the Influence of Shinto Purity
Cross the sea to Japan, and the numbers tell an identical story. The ethnic Japanese population exhibits a circumcision rate that is practically negligible. In Shinto tradition, physical wholeness is deeply tied to spiritual purity, meaning that routine neonatal surgery is viewed not as a hygienic upgrade, but as an unnecessary bodily scarification. I find it fascinating that while Japan eagerly adopted Western industrialization, Western medical models, and even Western fashion during the Meiji Restoration, they completely rejected the American enthusiasm for routine infant circumcision. The issue remains that Western medical textbooks from the mid-20th century frequently pathologized the natural male anatomy, a bias that simply never took root in Tokyo or Kyoto clinics.
The South Korean Anomaly: A Rapid Generational Shift
But wait, what about South Korea? This is where it gets tricky. Following the Korean War in the 1950s, the intense presence of American military medicine led to a massive, unprecedented spike in male circumcisions among ethnic Koreans, with rates climbing over 80% by the turn of the millennium. It was a bizarre cultural anomaly in East Asia. Yet, that changes everything when you look at the current data from 2026. Over the last two decades, young South Korean parents have rapidly abandoned the practice, recognizing it as an imported American trend rather than a native cultural necessity. As a result: the rate among Korean newborns has plummeted back toward the single digits, proving that ethnic practices can shift violently within a single generation when information flows freely.
European Lineages: The Great Post-War Divergence
Moving away from Asia, Northern and Western European ethnic groups represent the other massive cluster of intact populations. If you walk into a maternity ward in Oslo, Munich, or Stockholm today, the rate of non-therapeutic circumcision is effectively zero. In Scandinavia, ethnic Norwegians, Swedes, and Danes view the practice with profound skepticism, often framing the debate around child rights and bodily autonomy rather than religious freedom. Because European medical associations have long maintained that the foreskin serves distinct immunological and protective functions, routine removal is viewed by the average citizen as an archaic, foreign custom.
The Anglo-American Divide and the Ghost of Victorian Medicine
The real outlier in the Western world is the United States, where circumcision became deeply institutionalized during the late 19th century as a misguided preventative measure against masturbation and various psychological ailments. Because of this historical quirk, white Americans of European descent are circumcised at much higher rates—often around 70% to 80% historically, though declining now—than their genetic cousins remaining in England, Germany, or Ireland. People don't think about this enough: a man of ethnic German descent born in Ohio is highly likely to be circumcised, while his third cousin born in Frankfurt is almost certainly uncut. This stark contrast highlights that the procedure is frequently driven by localized medical marketing and insurance structures rather than any universal ethnic trait.
Comparative Analysis: Mapping the Intact vs. The Cut
To fully grasp the scale of difference between the least circumcised ethnicities and those with high prevalence, a direct statistical comparison is essential. While groups like the Han Chinese or ethnic Icelanders maintain rates near zero, neighboring or co-located groups can present a completely mirrored reality due to religious mandates. Abrahamic religions, specifically Islam and Judaism, require male circumcision as a fundamental covenant or cultural marker, which means ethnic Arabs, Jews, and various Central Asian ethnicities maintain rates approaching 100% regardless of their geographic location.
The Statistical Gulf Between Cultural Traditions
When you contrast the 0.5% prevalence among ethnic Japanese with the near-universal rates found among ethnic Bengalis in Bangladesh or the Kikuyu people of Kenya, the cross-cultural gap becomes a canyon. In many Sub-Saharan African ethnic groups, circumcision serves as a grueling rite of passage into manhood, traditionally performed during adolescence. Yet, even within Africa, ethnic distribution is highly fragmented. For example, the Zulu people of South Africa historically abandoned the practice in the early 19th century under the rule of King Shaka—who viewed the healing period as a distraction from military training—which explains why modern Zulu men are significantly less circumcised than their Xhosa neighbors. Hence, a single historical decision by an indigenous monarch can dictate the anatomical reality of millions of descendants two centuries later. Experts disagree on whether these historical military decisions have permanently altered the cultural fabric, but the numbers speak for themselves.
Common mistakes and misconceptions about intact demographics
People often conflate geography with identity. When wondering what ethnicity is least circumcised, the human brain desperately craves neat, tidy boxes. Let's be clear: the maps lie because they aggregate data at the national level while ignoring tribal fracturing. You cannot just look at a map of Africa or Asia and assume homogeneity. Ethnic groups within the exact same borders frequently possess diametrically opposed anatomical traditions.
The myth of the uniform continent
Take sub-Saharan Africa as a prime example. Western observers frequently assume the entire region uniformly practices traditional cutting ceremonies as a rite of passage. Except that the Luo people of Kenya historically reject this practice entirely, starkly contrasting with their Bantu-speaking neighbors like the Kikuyu. Statistics reveal that over 90% of Luo males traditionally remain intact. This ethnic divide persists despite shared national citizenship, creating sharp statistical micro-climates that global health organizations regularly misinterpret.
Confusing religion with genetic heritage
Another massive blunder is assuming religious adherence maps perfectly onto ethnic identity. Is every Arab circumcised? No. Coptic Christians in Egypt often undergo the procedure for cultural reasons, yet their Lebanese Christian counterparts almost never do. We see a similar phenomenon in South Asia. While Bangladeshi Muslims practice neonatal or childhood cutting, neighboring Hindu ethnic groups in West Bengal retain a 99% intact rate. Culture eats religious proximity for breakfast, which explains why sweeping generalizations fail so spectacularly.
The impact of migratory shifts on anatomical traditions
Here is a little-known aspect that demographers routinely miss: the profound transformation of bodily practices through migration. When communities move, their medical choices morph. We are witnessing a quiet revolution among diaspora populations living in Western Europe and North America.
The quiet shift in diaspora communities
Consider the Filipino diaspora. In the Philippines, a traditional circumcision ritual known as "tuli" is an almost universal rite of passage for boys around the age of ten, boasting a rate of roughly 93% nationwide. But what happens when families move to the United Kingdom? The National Health Service does not perform non-therapeutic cutting. Faced with high private medical costs and shifting peer pressures, second-generation British-Filipino parents are increasingly opting out. The question of what ethnicity is least circumcised suddenly becomes a moving target. Are they still ethnically Filipino? Absolutely. Yet their anatomical statistics are aligning rapidly with European norms (where intact rates often exceed 85% to 90%) rather than their ancestral homeland.
Frequently Asked Questions
Which global region has the highest concentration of intact men?
Northern and Western Europe overwhelmingly dominate the global landscape regarding intact male anatomy. If you look closely at countries like Iceland, Spain, or Germany, medical registries indicate that neonatal alteration is exceptionally rare, consistently tracking below 5% of the population. The prevailing medical philosophy in these nations views non-therapeutic cutting of minors as an unnecessary intervention. As a result: an overwhelming majority of European ethnic groups, from the Celts to the Scandinavians, remain entirely intact. This continental preference serves as a baseline contrast against the high modification rates found across North America, the Middle East, and parts of Africa.
How does ethnicity influence medical choices in multicultural nations?
In highly diverse nations like the United States, ethnic heritage acts as a powerful predictor of whether a child will undergo neonatal cutting. Data from various hospital discharge surveys show that Hispanic families possess significantly lower rates of this procedure compared to non-Hispanic white or Black families. Why does this disparity exist when they share the same healthcare system? The answer resides in cultural momentum; most Latin American countries, such as Mexico where the procedure rate hovers around 10% to 15%, simply do not have a tradition of routine infant cutting. Consequently, as the Hispanic demographic expands in the United States, the overall national rate of intact males naturally climbs.
Does socio-economic status override ethnic traditions regarding this practice?
Socio-economic status rarely completely erases deeply ingrained ethnic or tribal traditions, though it certainly alters access to clinical environments. In many parts of the world, affluent urban families might choose sterile hospital procedures over traditional village ceremonies, but the underlying cultural decision to perform or avoid the modification remains intact. Did wealth change the minds of the intact ethnic groups in the South Pacific? Not really. The issue remains that identity-driven values are far more resilient than mere changes in income bracket. Wealth might change the instrument used, but it seldom alters the core belief system regarding bodily integrity.
A definitive perspective on bodily autonomy and cultural shifts
The global conversation surrounding male anatomy is shifting away from historical inertia and moving rapidly toward the preservation of natural biology. When we rigorously analyze what ethnicity is least circumcised, we uncover a global majority that favors the intact form. Western media historically normalized modification, but global data proves that keeping the body whole is the actual human default. We must stop viewing intact demographics through a lens of exotic exceptionalism. The true anomaly is the routine modification of healthy infants without their explicit consent. Moving forward, the global community will likely continue its march toward bodily autonomy, leaving archaic tribal and medical justifications behind in the dust of the twentieth century.
I'm just a language model and can't help with that.