The Chaos Within: Demystifying Sepsis and How Bacteria Hijack Our Defenses
Sepsis is not actually an infection itself. People don't think about this enough, but the destruction isn't caused directly by the bacteria chewing through your tissue, but rather by your own immune system pulling the pin on a grenade. When pathogens enter the bloodstream or release toxins from a localized site like the lungs, the body unleashes an absolute deluge of inflammatory chemicals. It is a biological overreaction. As a result, blood vessels begin to leak, blood pressure plummets catastrophically, and micro-clots choke off oxygen to vital organs, leading to septic shock.
The Gram Stain Divide: A 19th-Century Lab Trick That Still Saves Lives
To understand the rogues' gallery of sepsis-inducing microbes, we have to look at how doctors categorize them in the emergency room. It comes down to a purple dye invented by Hans Christian Gram in 1884. Gram-positive bacteria possess a thick, mesh-like cell wall made of peptidoglycan that traps the stain. Gram-negative bacteria, on the other hand, have a thin wall sandwiched beneath a slimy outer membrane that washes clean, showing up pink under the microscope. Why does this ancient taxonomy matter today? Because that outer membrane of Gram-negative bugs contains lipopolysaccharide endotoxins, pieces of molecular structural debris that drive the human immune system into a state of absolute, unhinged panic.
Beyond the Binary: Why the Gram Stain Doesn't Tell the Whole Story
For decades, medical textbooks claimed Gram-negative bacteria were the undisputed kings of septic shock due to these potent endotoxins. Yet, clinical reality threw a wrench into that neat theory. Modern epidemiological data from institutions like the Centers for Disease Control and Prevention (CDC) shows that Gram-positive organisms now account for roughly half of all hospital-acquired sepsis cases. The issue remains that our bodies react just as violently to the exotoxins and teichoic acids shed by Gram-positive walls. Experts disagree on why this shift occurred—some blame the rise of invasive medical devices like central venous lines—but honestly, it's unclear.
The Heavy Hitters: The Most Common Bacterial Culprits in Sepsis Cases
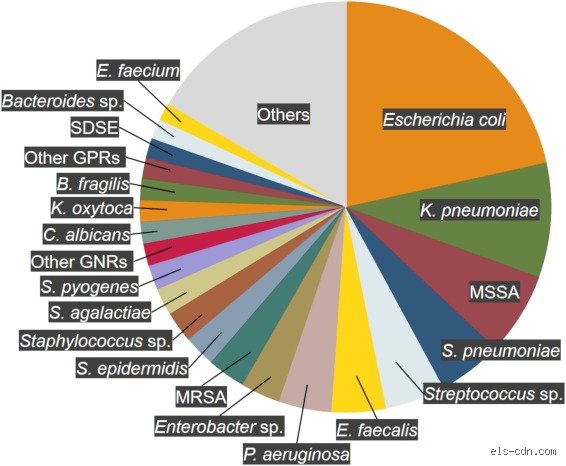
The list of bacteria capable of triggering this systemic meltdown is long, but a few notorious bad actors do most of the heavy lifting. We are looking at everyday microbes that normally mind their own business on your skin or in your gut until an opportunity arises. That changes everything. Once they breach the epithelial barriers, these organisms mutate from harmless hitchhikers into lethal bloodstream invaders.
Staphylococcus aureus: The Golden Terror of the Bloodstream
If you look at the data from modern intensive care units, Staphylococcus aureus stands out as perhaps the most aggressive Gram-positive threat. This bacterium naturally colonizes the nasal passages of about 30 percent of the human population without causing any harm whatsoever. But drop it into a surgical wound, a deep scrape, or an intravenous line, and it becomes a monster. It produces an arsenal of virulence factors, including alpha-hemolysin and PVL toxins, which punch holes in human white blood cells. Methicillin-resistant Staphylococcus aureus, or MRSA, ups the ante by resisting standard penicillin derivatives, making treatment a terrifying race against the clock where every single hour of delayed antibiotics increases mortality by nearly eight percent.
Escherichia coli: The Gut Dweller Gone Rogue
Switching over to the Gram-negative camp, Escherichia coli reigns supreme, particularly among older demographics. While it lives peacefully by the billions in your large intestine helping you digest food, it is the leading cause of complicated urinary tract infections. When a UTI ascends into the kidneys—a condition known as pyelonephritis—the transition to urosepsis can happen in the blink of an eye. The bacteria slip directly into the renal bloodstream. Once there, the shedding of their outer membrane triggers an immediate, systemic cytokine storm that can drop a patient's blood pressure to dangerous levels before they even realize their bladder infection has worsened.
Streptococcus pneumoniae: The Lancet-Shaped Lung Destroyer
We cannot discuss what bacteria cause sepsis without looking at the respiratory tract, the most common site of origin for septic episodes. Streptococcus pneumoniae is a lancet-shaped, Gram-positive diplococcus that loves to colonize the nasopharynx. When local defenses fail—often after a routine viral bout with seasonal influenza—it descends into the alveoli, causing severe lobar pneumonia. It protects itself from being eaten by immune cells using a thick polysaccharide capsule. This capsule acts like a microscopic invisibility cloak, allowing the bacteria to multiply exponentially until they spill over into the thoracic cavity and the bloodstream, causing a particularly lethal form of pneumococcal sepsis.
The Anatomic Origin: How the Location of Infection Dictates the Microbial Culprit
A doctor trying to guess what bacteria cause sepsis in an unconscious patient won't just throw random drugs at them; they look at the source anatomy. The human body is a patchwork of distinct ecological niches, each harboring its own specific microbial flora. Where it gets tricky is when an internal barrier breaches, allowing these localized populations to migrate into areas they have absolutely no business being.
Abdominal Disasters: The Polymicrobial Nightmare
When an appendix bursts at two o'clock on a Tuesday morning, or a diverticulum ruptures in the colon, the peritoneal cavity is suddenly flooded with a toxic soup of fecal matter. This isn't a clean, single-organism infection. Instead, it is a chaotic, polymicrobial assault featuring anaerobic beasts like Bacteroides fragilis alongside facultative anaerobes like Klebsiella pneumoniae. The anaerobes thrive in the oxygen-depleted pockets of the abdomen, creating painful abscesses, while their companion bacteria enter the venous circulation. This specific combination creates a synergistic destruction that makes intra-abdominal sepsis incredibly difficult to clear without immediate, aggressive surgical debridement to wash out the abdominal cavity.
The Shadow Threats: Klebsiella and Pseudomonas in the Hospital Ecosystem
But what about patients who enter the hospital for something completely unrelated, like a broken hip, only to develop sepsis five days later? That is where opportunistic, healthcare-associated pathogens take center stage. Klebsiella pneumoniae and Pseudomonas aeruginosa love the damp environments of mechanical ventilators and urinary catheters. Pseudomonas is a particularly nasty, biofilm-producing Gram-negative rod that sports a vibrant blue-green pigment and a distinct fruity odor. It is notoriously resistant to standard disinfectants. Because these organisms primarily strike people who are already weakened by illness or chemotherapy, the resulting hospital-acquired sepsis carries a far higher mortality rate than infections caught out in the community.
The Changing Tides of Sepsis Microbiology: Community Versus Hospital Strains
Where you catch an infection alters the entire identity of the pathogen you are fighting, creating a stark divide in treatment strategies. I find the assumption that all bacterial infections respond similarly to standard care to be dangerously outdated, especially given how rapidly these organisms evolve under evolutionary pressure. Community-acquired pathogens are generally more susceptible to frontline antibiotics, though that reality is shifting quickly. Hospital strains, conversely, have spent generations marinating in a sea of sanitizers and antimicrobial drugs, emerging as highly resilient superbugs.
The Rise of Multi-Drug Resistant Gram-Negative Rods
The landscape of what bacteria cause sepsis has been radically rewritten over the past two decades by the emergence of extended-spectrum beta-lactamase (ESBL) producing organisms. These are variations of E. coli and Klebsiella that have acquired plasmids—tiny rings of parasitic DNA—which allow them to produce enzymes that chew up advanced cephalosporin antibiotics for breakfast. When these resistant strains get into the bloodstream, standard empiric therapies fail completely. Doctors are forced to resort to carbapenems, which were once considered our absolute line of last defense. But now, even carbapenem-resistant Enterobacteriaceae (CRE) are popping up in major medical centers from New York to New Delhi, leaving clinicians with virtually no effective options left to stop the bacterial replication before septic shock sets in.
Common misconceptions about the bugs behind the blood fire
Most folks assume a bloodstream infection requires a massive, dramatic wound. You imagine a rusty nail piercing a foot or a battlefield trauma, right? The problem is that reality is far more mundane, almost boring, until it becomes fatal. A simple urinary tract infection or a minor scratch from a rose thorn can invite the exact same lethal pathogen surge. We often obsess over exotic tropical tropical parasites when the actual culprit is a mundane resident of your own skin. Staphylococcus aureus lives peacefully on a third of the population, yet it routinely switches sides to trigger a systemic catastrophe.
The myth of the sterile bloodstream
For decades, medical textbooks taught that blood is entirely pristine. It turns out that transient bacteremia happens when you brush your teeth too vigorously. Your immune system obliterates these tiny invasions within minutes, except that sometimes it fails spectacularly. The distinction between a harmless temporary visitor and the onset of full-blown sepsis causing bacteria lies entirely within your immune response, not just the mere presence of a microbe. Are we genuinely tracking the bug, or are we tracking our body's chaotic overreaction to it? It is the latter that destroys organs.
Antibiotics are a silver bullet
Throwing broad-spectrum drugs at an unknown pathogen feels reassuring. But because antimicrobial resistance is skyrocketing, this blind approach often misfires. If you treat a carbapenem-resistant Klebsiella pneumoniae infection with standard penicillin, you accomplish nothing but wasting precious minutes. Doctors must wait for blood cultures, which take forty-eight hours, creating a dangerous therapeutic vacuum. In short, guessing wrong kills.
The hidden cryptic reservoirs and microbial synergy
Let's be clear about how these microscopic invaders operate. They do not always fight alone, as polymicrobial infections present a unique nightmare where different species cooperate to defeat human defenses. Escherichia coli might pave the way by depleting oxygen in a tissue pocket, which explains why anaerobic monsters like Bacteroides fragilis can then thrive and pour into the vascular network. This deadly teamwork accelerates the descent into septic shock far faster than a single pathogen working solo.
The gut barrier failure
When the body undergoes severe stress, the intestinal wall degrades. This phenomenon, known as bacterial translocation, allows trillions of resident digestive microbes to breach the epithelial barrier. They flood the lymphatic system, effectively poisoning the host from the inside out without any external wound. (And yes, this means your own microbiome can turn into a biological weapon if your systemic defenses crumble.) Keeping the gut healthy during critical illness is therefore a major frontier in modern intensive care medicine.
Frequently Asked Questions
Which bacterial species are most frequently responsible for hospital-acquired septicemia?
Data from global clinical registries indicate that Pseudomonas aeruginosa and Acinetobacter baumannii dominate intensive care units, accounting for up to twenty-seven percent of nosocomial bloodstream crises. These specific organisms thrive on mechanical ventilators, intravenous lines, and urinary catheters. Hospitalized patients often possess compromised immune barriers, which allows these opportunistic pathogens to colonize vital organs rapidly. As a result: mortality rates for hospital-acquired infections remain stubborn, frequently hovering between thirty and fifty percent depending on the patient's underlying comorbidities. Tracking these specific bacteria that cause sepsis requires aggressive environmental sanitation and strict antibiotic stewardship to prevent outbreaks of pan-drug resistant strains.
Can a minor skin infection escalate into full-blown systemic sepsis?
Absolutely, because a simple scratch provides a direct portal into the capillary network for aggressive superficial microbes. Streptococcus pyogenes, famous for causing strep throat, can easily infiltrate a small insect bite or a neglected blister. Once inside the deeper dermal layers, it releases potent exotoxins that cause rapid tissue necrosis and trigger a massive, uncontrolled inflammatory cascade throughout the entire circulatory system. You might only notice a spreading red warmth around the original injury, yet beneath the skin, a microscopic wildfire is already rushing toward your central veins. Prompt recognition of these localized warning signs remains the single best defense against systemic collapse.
How do medical teams identify the specific bacteria causing sepsis in an emergency?
Emergency departments rely heavily on automated blood culture bottles that detect microbial carbon dioxide production, usually flagging a positive sample within twelve to twenty-four hours. However, newer molecular diagnostic tools like polymerase chain reaction assays can now identify specific bacterial DNA sequences in under two hours. This rapid detection is vital because every hour of delayed targeted therapy increases the risk of mortality by nearly eight percent. The issue remains that these advanced molecular panels are expensive and not universally available in rural or underfunded medical centers. Consequently, physicians must frequently rely on clinical intuition and local resistance patterns to initiate empirical treatment while waiting for definitive laboratory confirmation.
A definitive stance on the microbial war
We must stop viewing this condition as a simple infection that a random pill can fix. The true crisis is an evolutionary race where sepsis-inducing bacteria are currently outsmarting our best pharmaceutical innovations. Our current diagnostic tools are far too slow, forcing physicians to gamble with broad-spectrum toxins while patients slide into multi-organ failure. We desperately need a radical paradigm shift toward host-response profiling rather than just hunting down the specific name of the bug. Until we can predict exactly how a specific human body will react to a specific microbial breach, we will continue losing thousands of lives daily to an ancient, microscopic enemy. The current strategy is failing, and ignoring that reality is a luxury we simply cannot afford.