Beyond the Basics: Why the Standard Definition of Sepsis Fails Patients in the ER
For decades, the medical establishment viewed sepsis as a simple, linear progression of blood poisoning. We were taught that bacteria invaded the bloodstream, threw a party, and the body reacted with inflammation. Except that the reality is infinitely more chaotic. Sepsis is not actually an infection itself; rather, it is a life-threatening organ dysfunction caused by a dysregulated host response to an infection. It is your own defense system burning down the house to catch a thief. And honestly, it is unclear why two patients of identical age and health can contract the exact same urinary tract infection, yet one walks away with a routine prescription while the other ends up on life support within forty-eight hours.
The Lethal Shift from Localized Infection to Systemic Anarchy
Think of a localized infection like a small kitchen fire. Your immune system usually deploys local firefighters—white blood cells—to douse the flames. But in septic patients, the body panics and drops a nuclear bomb on the entire city. The endothelium, that microscopic inner lining of your blood vessels, begins to leak fluid into surrounding tissues. This causes blood pressure to plummet catastrophically, a state known clinically as septic shock. Why does this happen? The thing is, our biological alarm system lacks a nuance dial, meaning the chemical cascade intended to heal actually ends up suffocating vital organs by cutting off their oxygen supply.
The Statistical Toll of a Medical Emergency That Mocks the Clock
The numbers coming out of global health registries are downright terrifying. According to data published by the World Health Organization, sepsis affects an estimated 49 million people globally each year, leading to approximately 11 million deaths. That changes everything when you realize it represents nearly one in five deaths worldwide. In American hospitals, a landmark study tracking ICU admissions found that the risk of mortality increases by roughly 7.6% for every single hour that antibiotic treatment is delayed once hypotension sets in. We are far from achieving a standardized, foolproof diagnostic test, which explains why clinical observation remains our sharpest weapon.
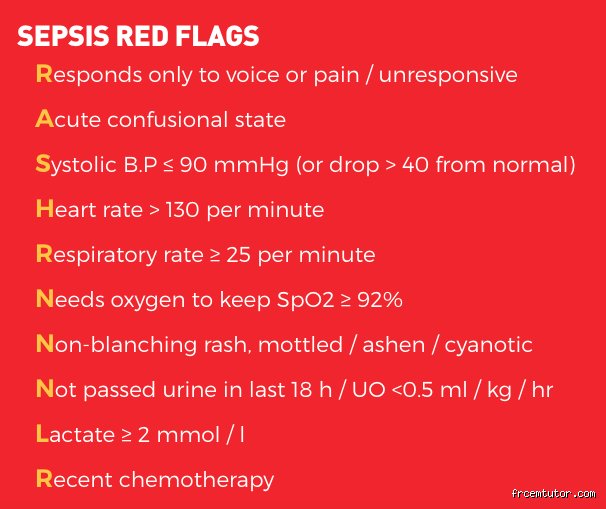
The First Warning Sign: Uncontrollable Rigors and the Deceptive Illusion of Fever
People don't think about this enough, but a thermometer can be a terrible liar. When evaluating what are three red flags for sepsis, the traditional expectation is a raging, sweat-inducing fever. Yet, the true red flag is often the exact opposite: uncontrollable, teeth-chattering shivering, sometimes accompanied by an abnormally low body temperature. This phenomenon, known medically as hypothermia in sepsis, frequently targets the elderly and infants. When a patient at the Royal Infirmary in Edinburgh back in 2022 presented with a temperature of just 35.5 degrees Celsius alongside violent tremors, rookie triagers suspected exposure, but it was actually a full-blown pneumococcal septic invasion.
The Physiology Behind the Shiver That Will Not Stop
Why do you shake so violently when your body is under systemic siege? Your brain's hypothalamus acts as the central thermostat, and during a severe infection, bacterial endotoxins warp its settings. The brain suddenly decides the body is freezing, even if the room is boiling. Consequently, your muscles contract rapidly to generate heat, creating those deep, exhausting rigors that no amount of heavy blankets can soothe. Where it gets tricky is that this massive muscular exertion consumes enormous amounts of oxygen, further draining an already exhausted circulatory system.
Why Hypothermia is Far More Sinister Than a Raging Fever
A high fever means your immune system is throwing punches and fighting back hard. But what happens when the body's temperature drops below 36 degrees Celsius during an infection? That is a sign of immunoparalysis. The system is crashing, unable to even mount a basic thermoregulatory defense. Medical data shows that septic patients who exhibit hypothermia have a significantly higher mortality rate than those with a high fever. It is a quiet, cold shutdown that catches family members completely off guard because they assume the absence of a hot brow means the danger has passed.
The Second Warning Sign: Sudden Altered Mental Status and Acute Cognitive Eclipse
Imagine your normally sharp, fiercely independent seventy-year-old grandmother suddenly forgetting where she is, or perhaps struggling to string a coherent sentence together during Sunday dinner. You might initially suspect a stroke, or maybe a sudden onset of dementia. But acute confusion, lethargy, or profound disorientation is a massive, immediate red flag for sepsis that requires an emergency room evaluation. This condition, formally termed sepsis-associated encephalopathy, affects up to 70% of severely septic patients and often manifests long before any drop in blood pressure occurs.
How Microscopic Brain Inflammation Mimics Sudden Dementia
The blood-brain barrier is supposed to be an impenetrable fortress keeping toxins out of your central nervous system. But during sepsis, the systemic storm of pro-inflammatory cytokines breaches these walls. As a result: microscopic blood clots form in the cerebral capillaries, astrocytes swell, and normal neurotransmitter signaling breaks down completely. I have watched patients change from perfectly lucid individuals to hallucinating, terrified individuals within a span of four hours. It is not a psychological break; it is chemical warfare inside the cerebral cortex caused by a distant infection, like an undiagnosed kidney infection or a neglected scrape from gardening.
Spotting the Difference Between Routine Delirium and Septic Encephalopathy
But how do we differentiate this from standard age-related confusion or a mild urinary tract infection side effect? The issue remains one of velocity and scale. Septic cognitive decline is aggressive, frequently paired with extreme lethargy where the patient can barely keep their eyes open. If they are sleeping constantly and cannot answer basic questions about the year or their name, the brain is actively suffocating due to poor perfusion. Never dismiss sudden behavioral changes as just old age or fatigue, because that assumption is precisely how early-stage intervention opportunities slip away.
The Structural Divergence: Sepsis Red Flags Versus Standard Inflammatory Responses
It is easy to panic and think every case of the flu is a death sentence, which brings us to a critical clinical distinction. We must contrast true septic red flags against the standard Systemic Inflammatory Response Syndrome, or SIRS. If you go for a vigorous five-mile run in July, your heart rate will skyrocket and you will breathe heavily, yet you are obviously not septic. Your body is simply adapting to metabolic demand. Sepsis, however, breaks the rules of homeostatic compensation, forcing the body into a destructive loop where the cardiorespiratory system accelerates frantically but fails to deliver oxygen to tissues.
Comparing Normal Immune Fighting Metrics Against Septic Breakdown
Let us look at how a healthy immune response differs from a septic trajectory. When you catch a standard viral bug, your heart rate might tick up to 90 beats per minute to help move white blood cells around the circuit. In contrast, a septic pulse often blasts past 110 beats per minute while the blood pressure simultaneously sinks below 100 mmHg systolic. This specific, lethal decoupling of heart rate and blood pressure is the hallmark of circulatory collapse. The heart is pumping furiously, desperately trying to fill a vascular system that has suddenly lost its tone and become as porous as a sponge.