Every desperate late-night Google search by terrified parents usually leads to this exact, loaded question. There is a multi-million dollar industry capitalizing on that precise panic, promising total reversals through hyperbaric oxygen chambers or restrictive diets. I find this marketing predatory. The reality is far more nuanced, grounded in biology rather than miracle cures. We are talking about an intricate tapestry of genetic predispositions and neural connectivity that begins long before a child takes their first breath.
The Diagnostic Shift: Why We No Longer Talk About Curing the Spectrum
Autism Spectrum Disorder, as codified in the DSM-5-TR, is defined by persistent deficits in social communication and restricted, repetitive patterns of behavior. For decades, the medical establishment viewed these traits as static deficits. That changes everything when you look at modern neurology. The old paradigm treated autism like an invader, an external illness that could perhaps be purged or eradicated if caught early enough.
From Kanner to the Spectrum Continuum
Leo Kanner first identified "infantile autism" in Baltimore back in 1943, describing children with an powerful desire for aloneness. But his rigid definition caused decades of misunderstanding. Today, clinicians recognize that the presentation of neurodivergence is wildly heterogeneous. One child might be entirely non-verbal, requiring 24-hour assistive care; another might graduate from MIT while struggling immensely with sensory processing or the unwritten rules of office politics. Because the spectrum is so vast, looking for a singular mechanism to reverse autism if caught early is a fool's errand. Honestly, it's unclear if a single biological mechanism even exists across all these variations.
The Problem With the Optimal Outcome Metric
In 2013, a groundbreaking study by Dr. Deborah Fein at the University of Connecticut tracked a cohort of individuals who had documented, verified histories of early-childhood autism but no longer met the criteria as young adults. They called this optimal outcome. But did these individuals actually reverse autism? Except that when researchers looked closer, many of these kids still retained subtle differences in executive functioning and faced heightened risks for anxiety. The underlying neurology remained fundamentally unique; the outward behavior had simply been masterfully socialized.
The Science of the Infant Brain: Plasticity and Synaptic Pruning
If we want to understand why early intervention carries such immense weight, we have to look closely at the sheer, chaotic velocity of the developing infant brain. At birth, a baby has roughly 86 billion neurons. By age two, the brain has formed trillions of synapses—far more than it actually needs. Then comes the cleanup crew.
Hyper-Connectivity and the Pruning Deficit
In neurotypical development, a process called synaptic pruning kicks into high gear, systematically eliminating weak or redundant neural connections to streamline communication. Where it gets tricky is that post-mortem brain studies, like those conducted at Columbia University Medical Center in 2014, reveal that autistic children often exhibit a distinct lack of this natural pruning. Their brains retain an overabundance of synapses. Imagine trying to listen to a single violin concerto, but you are standing in a room where 50 different stereos are blasting 50 different radio stations simultaneously. That is the sensory reality of a hyper-connected cortex. Can an early behavioral therapy physically force the brain to prune these excess synapses? We are far from it, biologically speaking.
The Window of Vulnerability and Opportunity
Yet, the infant brain possesses an astonishing degree of neuroplasticity, a malleable state where experiences directly sculpt physical architecture. Between the ages of 0 and 3, the brain is hyper-reactive to environmental input. This is why interventions like the Early Start Denver Model (ESDM)—which blends behavioral principles with developmental, relationship-based approaches—show such profound efficacy. By engaging a toddler in highly structured, play-based interactions during this critical window, therapists can effectively bypass damaged or inefficient neural pathways, building sturdy alternative routes for language and social connection before the brain's architecture hardens. People don't think about this enough: you aren't changing the child's genetic makeup, but you are radically altering how their brain processes the world around them.
Decoding the True Impact of Early Intervention Protocols
When clinicians talk about mitigating the presentation of symptoms, they generally point to a few gold-standard methodologies that have undergone rigorous peer review. The goal is never to erase the child's identity, but rather to minimize the disabling aspects of their condition.
Applied Behavior Analysis vs. Developmental Models
For a long time, Applied Behavior Analysis (ABA) reigned supreme as the only insurance-reimbursable therapy for autism. Developed by B.F. Skinner’s disciple Ivar Lovaas at UCLA in the 1960s, early iterations used intense, repetitive drills—sometimes up to 40 hours a week—to condition children out of repetitive movements like hand-flapping. It worked to modify behavior, but the issue remains that many adult self-advocates now look back on those intensive, compliance-based methods as deeply traumatic. Contrast that with modern, naturalistic developmental behavioral interventions (NDBIs) which lean into a child’s natural motivations. If a two-year-old is obsessed with spinning the wheels on a toy truck, a skilled therapist won't slap their hand away; instead, they will sit on the floor, spin a wheel too, make eye contact, and turn it into a shared, communicative game. This subtle shift from suppression to connection is what drives genuine, meaningful neuroplastic change.
The Toddler Developmental Screening Revolution
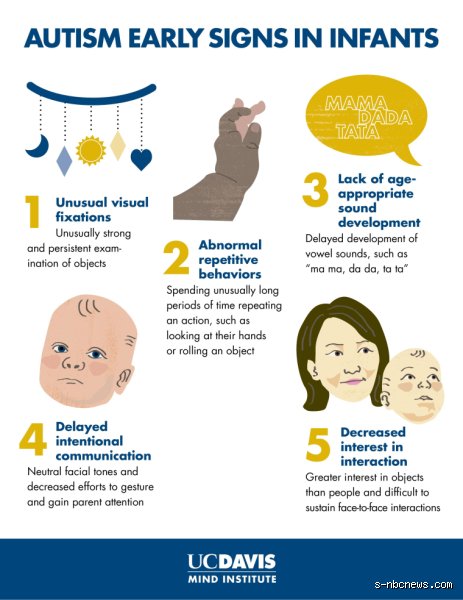
Waiting until a child fails to speak at age three is a massive administrative failure. Pediatricians now utilize tools like the Modified Checklist for Autism in Toddlers (M-CHAT) at the 18-month checkup to flag subtle indicators long before overt delays manifest. A lack of proto-imperative pointing, an inability to follow a parent's gaze, or a failure to respond to one's own name are all early smoke signals. As a result: intervention can begin when the nervous system is at its most receptive, dramatically increasing the odds that a child might eventually move outside the diagnostic boundaries of the spectrum entirely.
The Genetic Underpinnings: Why Erasure is Biologically Flawed
To believe you can reverse autism if caught early is to misunderstand the profound genetic architecture that dictates human development. Autism is not a virus that a child catches in toddlerhood; it is baked into their DNA long before the first ultrasound.
The Polygenic Architecture of Neurodivergence
Unlike Huntington’s disease, which can be traced to a single mutated gene, autism is fiercely polygenic. Large-scale genomic sequencing projects, such as the SPARK study which analyzed tens of thousands of families, have identified over 100 high-confidence autism risk genes, alongside hundreds of other smaller genetic variants. Some of these genes govern the way ion channels operate in neurons; others control the synthesis of neurotransmitters at the synaptic cleft. It is an incredibly complex web. How do you reverse a condition that is written into the very code of a person's cellular biology? The thing is, you simply cannot rewrite that fundamental code through behavioral therapy or dietary adjustments.
Epigenetics and Environmental Triggers
Of course, genetics do not exist in a vacuum. The field of epigenetics examines how environmental factors can flip specific genetic switches on or off during gestation. Maternal immune activation during pregnancy, advanced paternal age, and exposure to specific environmental toxins have all shown statistical correlations with increased autism rates. But these factors merely influence how the brain's blueprint is executed. By the time a child is born, the structural foundation of their nervous system has already been laid down. You can alter the interior design of that house through decades of hard work and therapy, but you aren't going to tear down the load-bearing walls without collapsing the entire structure.