The Shocking Reality of Non-Pregnancy Lactation and Galactorrhea
The human body loves a good loophole. When we talk about how a woman can get milk in her breast without pregnancy, we are usually looking at one of two distinct pathways: galactorrhea, which is an inappropriate, spontaneous leakage of milk, or induced lactation, which is a deliberate, highly orchestrated effort to mimic the hormonal shifts of birth. Let's be honest, the idea that a non-pregnant body can just start producing milk sounds like science fiction. But it happens. And it happens far more frequently than the medical community’s historically dismissive attitude would suggest.
Unmasking Galactorrhea vs. Induced Lactation
Galactorrhea is not a disease in itself; rather, it is a symptom, a smoke signal from the endocrine system indicating that your internal chemistry has gone off-script. It is characterized by a milky, multi-duct bilateral breast discharge in individuals who are not actively pregnant or breastfeeding. I find that patients often panic, immediately jumping to conclusions about malignancy, yet galactorrhea is fundamentally an endocrine issue, not a structural breast disease. On the flip side, induced lactation is an intentional, manual process. Think of adoptive mothers or intended parents via surrogacy who utilize a combination of mechanical pumping and pharmacological assistance to feed their newborns. The milk is structurally identical, but the road to getting there is completely different.
The Historical Blind Spot in Women's Endocrine Health
For decades, women experiencing spontaneous lactation were met with blank stares in clinics, or worse, immediate psychiatric referrals. A landmark 1974 clinical review by Dr. Guyda et al. finally shed light on the hyperprolactinemia connection, proving that this wasn't psychological hysteria but a measurable, biochemical reality. People don't think about this enough, but our understanding of non-puerperal lactation was severely limited until the widespread availability of serum prolactin assays in the late twentieth century. Before that? Pure guesswork. Which explains why so many historical cases went entirely undocumented or misdiagnosed as phantom pregnancies.
The Delicate Endocrine Architecture Governing Milk Production
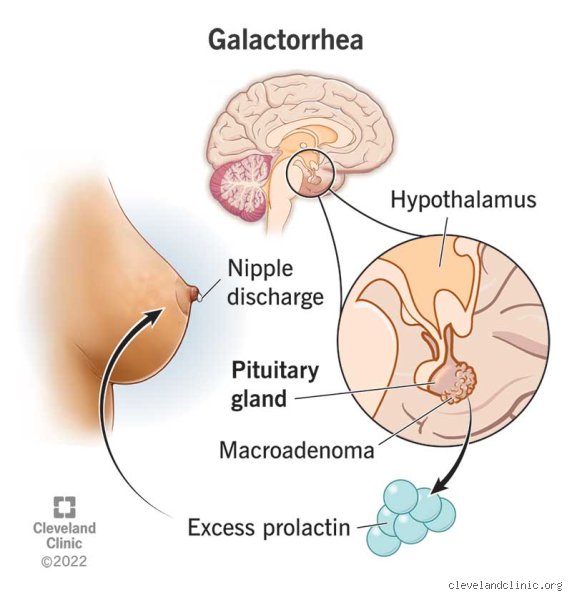
Where it gets tricky is the delicate ballet of hormones required to initiate and sustain milk production. The primary driver here is prolactin, a polypeptide hormone synthesized and secreted by lactotroph cells in the anterior pituitary gland. Under normal, non-lactating conditions, your brain keeps prolactin under a strict, heavy lock and key.
The Prolactin-Dopamine Tug-of-War
Dopamine is the bad guy here—or the fun killer, depending on your perspective. Secreted by the hypothalamus, dopamine acts as the primary prolactin-inhibiting factor (PIF) via the tuberoinfundibular pathway. It binds to D2 receptors on lactotrophs, effectively shutting down prolactin secretion. But what happens if you disrupt that pathway? The brake pedal is lifted. Prolactin levels spike, rushing toward the mammary epithelial cells to stimulate transcription of milk proteins like casein and alpha-lactalbumin. It is a fragile equilibrium. A tiny shift in brain chemistry, and suddenly, the system is flooded with milk-producing signals.
The Estrogen and Progesterone Paradox
During a typical pregnancy, massive surges of estrogen and progesterone from the placenta prepare the breast tissue, causing the alveolar buds to branch and mature into functioning lobules. Yet, these high steroid levels simultaneously block prolactin from actually triggering milk letdown. It is only when the placenta detaches, causing estrogen and progesterone levels to plummet off a cliff, that prolactin can finally do its job. In a non-pregnant woman, however, chronically elevated estrogen—say, from an ovarian cyst or specific hormone therapies—can paradoxically over-stimulate the pituitary gland, leading to hyperprolactinemia once those levels fluctuate. The thing is, your breasts don't always need the full nine months of preparation to start leaking; sometimes, a chaotic hormonal spike is more than enough.
Pharmacological Catalysts: Medications That Trigger Lactation
Can a woman get milk in her breast without pregnancy simply by changing her daily prescriptions? Absolutely. In fact, drug-induced galactorrhea is one of the most common diagnoses in modern endocrinology, accounting for an estimated 20% to 30% of clinical cases. When exogenous substances interfere with the delicate dopamine-prolactin axis, the body responds exactly as if it were preparing to nurse.
Antipsychotics and the Dopamine Blockade
First-generation antipsychotics like haloperidol, alongside atypical antipsychotics such as risperidone and paliperidone, are notorious for this. Because these medications work by aggressively blocking dopamine D2 receptors to manage psychiatric symptoms, they inadvertently unleash prolactin. Imagine a dam bursting. Without dopamine to hold it back, serum prolactin levels can rocket from a normal baseline of under 25 ng/mL to well over 100 ng/mL within days of starting treatment. A patient in Chicago recently documented her experience of waking up to damp sheets just three weeks after adjusting her risperidone dosage—that changes everything when you are trying to manage mental health without physical surprises.
Gastrointestinal Motility Agents and Antidepressants
It is not just heavy psychiatric drugs either. Common GI medications, specifically metoclopramide (Reglan) and domperidone, are potent dopamine antagonists. Domperidone is so effective at crossing this threshold that it is routinely used off-label globally to deliberately induce lactation in adoptive mothers, despite regulatory caveats in certain jurisdictions. Furthermore, Selective Serotonin Reuptake Inhibitors (SSRIs) like sertraline and fluoxetine can alter synaptic serotonin levels, which indirectly inhibits dopamine neurons, leading to mild, spontaneous breast discharge. It’s a cascading biochemical domino effect.
Mechanical Stimulation and the Neuroendocrine Arc
But let's look at a completely non-chemical route. Can a woman get milk in her breast without pregnancy through purely physical means? Yes, because the body cannot always tell the difference between a medical pump, a romantic partner, or a poorly fitting sports bra.
The Intercostal Nerve Reflex
Physical stimulation of the nipple-areolar complex sends rapid afferent neural signals through the fourth, fifth, and sixth intercostal nerves directly to the paraventricular and supraoptic nuclei in the hypothalamus. This neural traffic does two things simultaneously: it suppresses dopamine release and triggers the release of oxytocin from the posterior pituitary. Oxytocin causes the myoepithelial cells surrounding the alveoli to contract, forcing any accumulated fluid down the lactiferous ducts. If this stimulation is frequent and vigorous enough—such as pumping every 2 to 3 hours around the clock—the pituitary gland adapts, ramping up prolactin production from scratch, even in a nulliparous woman. We are far from the realm of impossibility here; this is basic biological plumbing operating on a feedback loop.
Common mistakes and widespread misconceptions
The panic of the phantom tumor
You notice a white drop. Immediately, your mind sprints to the absolute worst-case scenario. Google told you it is a pituitary adenoma, a terrifying brain growth. Let's be clear: while prolactinomas do exist, they are rarely catastrophic. Fewer than 1% of galactorrhea cases stem from malignant conditions. Most people panic needlessly. The problem is that stress itself alters your endocrine chemistry. Cortisol spikes, disrupting your delicate hormonal equilibrium. You stir up a storm in a teacup. Stop squeezing your breasts to check if it stopped; mechanical stimulation actually signals your brain to produce more fluid.
The assumption of immediate infertility
Can a woman get milk in her breast without pregnancy and still conceive? Absolutely. Many mistakenly believe that non-puerperal lactation acts as a foolproof natural contraceptive. It does not. High prolactin can suppress ovulation, except that this suppression is wildly unpredictable. Approximately 30% of women with idiopathic galactorrhea maintain perfectly normal ovulatory cycles. Relying on fluid production to prevent pregnancy is reckless. You might end up expecting a baby while wondering why you already have milk.
Ignoring the pharmacy cabinet
People blame mystery illnesses. Yet, the true culprit often sits quietly on their nightstand. Common blood pressure medications, specific antidepressants, and even over-the-counter gastrointestinal pills can trigger spontaneous lactation. Metoclopramide is a classic example. But because these pills are familiar, we completely overlook them. We search for rare syndromes instead of checking the side effects of our daily prescriptions. It is a classic case of missing the forest for the trees.
An overlooked clinical reality: Induced adoptive lactation
The power of mechanical intent
There is a fascinating, deliberate side to this phenomenon. Adoptive mothers can intentionally induce milk production without ever being pregnant. It requires fierce dedication. By utilizing a strict regimen of mechanical pumping every three hours alongside specific galactagogues, women can stimulate the mammary glands. The issue remains that society views lactation as purely gestational. It isn't. The human body possesses a remarkable latent capacity to nurture. Around 55% of adoptive mothers who follow intensive protocols manage to produce a meaningful milk supply. Which explains why non-gestational lactation should be viewed with scientific awe rather than immediate medical alarm.
Frequently Asked Questions
Can stress alone cause a woman to get milk in her breast without pregnancy?
Yes, chronic psychological distress acts as a potent catalyst for spontaneous lactation. When your nervous system remains in a perpetual state of fight-or-flight, the hypothalamus struggles to regulate dopamine, the chemical responsible for keeping prolactin levels in check. Clinical data indicates that emotional trauma can elevate serum prolactin levels by up to 40% in otherwise healthy individuals. As a result: fluid emerges from the nipples without any underlying physical disease. It is a vivid physical manifestation of mental exhaustion, proving that your brain and breasts are deeply interconnected.
How long does non-puerperal lactation typically last?
The duration varies dramatically based entirely on the root cause. If the fluid stems from a specific medication, production usually ceases within two to three weeks after discontinuing the drug. Idiopathic cases—where doctors find absolutely no identifiable cause—can stubbornly persist for several years. (Yes, you read that right, years). In short, unless the mechanical stimulation of the nipple stops completely, the mammary glands might keep trickling indefinitely. If it lasts longer than six months without a clear trigger, a comprehensive endocrine panel is required.
When should non-gestational nipple discharge trigger an urgent doctor visit?
While most occurrences are benign, certain red flags demand immediate investigation. If the fluid is bloody, expressed from only one single duct, or accompanied by a hard, immovable lump, you must see a specialist. Statistics reveal that bloody unilateral discharge carries a 10% to 15% correlation with localized mammary pathologies, including intraductal papillomas. Colorless or milky fluid from both sides is usually hormonal. Is it worth ignoring a sudden change? Never, because pinpointing the exact etiology early saves you months of anxiety and guarantees proper targeted therapy.
An unyielding stance on non-gestational lactation
We must change how we talk about the female endocrine system. Idiopathic fluid production is treated like a bizarre medical failure, but it is actually a testament to human adaptability. Medical professionals frequently over-medicate patients who present with mild, harmless galactorrhea. Stop treating every single drop of non-gestational milk as a crisis that requires aggressive pharmaceutical intervention. If there is no tumor and no pain, we should stop pathologizing a body that is simply reacting to its environment. Let us accept that the boundary between maternal and non-maternal biology is far more fluid than traditional textbooks care to admit.