I have seen men agonize over this choice for months, often paralyzed by the sheer volume of conflicting data thrown at them by urologists and oncologists alike. It is a messy, deeply personal trade-off. We like to pretend medicine is a series of binary right-or-wrong answers, but here, the thing is that you are often choosing between two different versions of "difficult." One path involves the immediate trauma of the knife and the sudden, jarring shift in urinary control; the other is a slow burn, a series of appointments that might leave you feeling fine today but struggling with bowel issues three years down the line. We are far from a consensus on which is "objectively" superior because, honestly, it’s unclear if such a thing even exists when quality of life is so subjective.
The Biological Reality of Localized Prostate Cancer Treatment Options
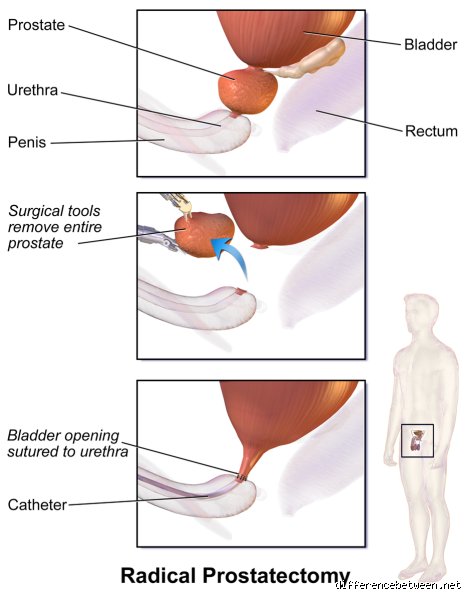
Before we can even talk about which is better, we have to look at what we are actually trying to accomplish with localized therapy. Surgery—specifically radical prostatectomy—is the literal extraction of the gland and the surrounding seminal vesicles. Since the early 1980s, when Dr. Patrick Walsh popularized nerve-sparing techniques at Johns Hopkins, the goal has been to save the delicate cavernous nerves responsible for erections. But the prostate is tucked away in a tiny, crowded pelvic space, surrounded by the bladder and the rectum, making it a high-stakes demolition job. If the surgeon misses even a few microscopic cells at the margin, the "cure" is incomplete.
Understanding the Mechanics of Radiation Therapy
Radiation takes the opposite approach by leaving the organ in place and using high-energy beams to shred the DNA of the cancer cells. This is not the blunt-force radiation of the 1970s; today, we use Intensity-Modulated Radiation Therapy (IMRT) or Stereotactic Body Radiotherapy (SBRT), which allows doctors to map the prostate in three dimensions. Why does that change everything? Because it allows for a higher dose of "killing power" to the tumor while attempting to spare the healthy bladder and rectal tissue nearby. Yet, despite the precision, the radiation still has to pass through healthy skin and muscle to reach its target, which explains why some men experience that "sunburn on the inside" feeling during their weeks of treatment.
The Role of PSA Monitoring After Intervention
People don't think about this enough: how we define "success" differs between the two methods. After surgery, your PSA (Prostate-Specific Antigen) should drop to undetectable levels—essentially zero—within six weeks. If it doesn't, or if it starts to creep up, we know immediately that something went wrong. Radiation is different. Because the prostate is still in your body, it continues to produce some PSA, and we look for a "nadir," or the lowest point, which can take two years to reach. This creates a strange, lingering anxiety for the radiation patient that the surgery patient often avoids, although the surgery patient has to deal with the immediate physical fallout of a catheter.
Surgical Intervention: The Case for Removing the Problem Entirely
There is a psychological comfort in knowing the cancer is in a jar in a pathology lab somewhere rather than still inside your pelvis. That is the primary driver for many men choosing the da Vinci robotic-assisted laparoscopic prostatectomy, which has become the gold standard in the United States since its FDA approval in 2000. But the issue remains that surgery is a massive physiological shock. You are under general anesthesia for three to four hours, and your body has to reroute your entire urinary system. The urethra, which used to run through the prostate like a straw through a donut, now has to be sewn directly to the bladder neck.
Immediate vs. Delayed Side Effects in the Surgical Group
If you go under the knife, you are essentially "front-loading" your misery. You wake up with a catheter, you deal with potential wound infections, and almost every man experiences stress urinary incontinence for at least a few months. It is the price of admission. But—and this is a big "but"—if you are young and otherwise healthy, surgery offers the benefit of keeping radiation in your back pocket as a "salvage" therapy if the cancer returns. You cannot easily do it the other way around; performing surgery on a prostate that has been previously radiated is like trying to cut through scarred, leathery tissue that doesn't heal well. Which explains why surgeons are often hesitant to operate on a failed radiation site.
The Statistical Reality of Cancer Control
Data from the ProtecT trial, published in the New England Journal of Medicine, followed over 1,600 men for a decade. The results were startling: there was no significant difference in prostate cancer mortality between surgery and radiation. Mortality was incredibly low—about 1% across the board. So, if the survival is the same, why do we even argue? Because while the survival was the same, the incidence of disease progression was slightly higher in the group that didn't have surgery. Does that mean surgery is better? Not necessarily, especially if that progression doesn't actually kill you or shorten your life. It just adds another layer of complexity to the decision-making process.
The Rise of Radiation: Is Non-Invasive Always Superior?
For the man who cannot afford six weeks of recovery or who has a heart condition that makes anesthesia risky, radiation is a godsend. There is no hospital stay, no incisions, and usually no catheter. You drive yourself to the clinic, lay on a table for fifteen minutes, and go get lunch. It sounds like a no-brainer, right? Except that radiation is a slow-acting treatment. The biological effect of the beams continues to evolve months and even years after the final session. This is where we see the late-term "rectal toxicity" or "radiation cystitis" that can cause bleeding or urgency long after you thought you were in the clear.
Proton Therapy and the Promise of Reduced Collateral Damage
We often hear about Proton Beam Therapy as the "next big thing." It uses heavy particles rather than X-rays, allowing the energy to stop abruptly at a specific depth—the "Bragg Peak"—theoretically sparing the organs behind the prostate. Marketing departments at major cancer centers love to tout this as the ultimate solution. Yet, the actual clinical data comparing protons to standard IMRT is still surprisingly thin when it comes to long-term cure rates. Is it worth the significantly higher cost? For some, the peace of mind is worth it; for others, it’s just another expensive piece of tech that hasn't quite proven it can outperform a skilled radiation oncologist with a standard machine.
The Hormonal Component: A Hidden Burden
Many men choosing radiation are surprised to find they also need Androgen Deprivation Therapy (ADT). This isn't part of the radiation itself, but a chemical castration designed to starve the cancer cells of testosterone, making them more vulnerable to the beams. If your cancer is high-risk, you might be on these drugs for eighteen months to three years. Imagine dealing with hot flashes, muscle loss, and a complete disappearance of libido while you are also trying to stay positive about your "non-invasive" treatment. Surgery rarely requires this hormonal heavy lifting upfront, which is a nuance that changes everything for men who value their hormonal vitality.
How Your Age and Comorbidities Tip the Scales
A 55-year-old marathon runner and a 78-year-old with type 2 diabetes are not looking at the same map. For the younger man, life expectancy is the dominant factor. He has thirty years of potential life ahead of him, meaning he has thirty years for a slow-growing cancer to eventually cause trouble. He also likely has a stronger pelvic floor, making recovery from surgical incontinence much faster. Conversely, for the older patient, the risks of a major operation might outweigh the benefits. If you have a significant cardiovascular history, the stress of surgery could be more dangerous than the cancer itself, hence the leaning toward radiation or even active surveillance.
Comparing the Impact on Sexual Function
Let's be blunt: both treatments are a disaster for your sex life, just in different ways. With surgery, the impact is immediate and mechanical. If those nerves are bruised or cut, the "wiring" is gone. With radiation, the decline is often gradual. You might be fine for the first year, but as microvascular damage sets in over the following thirty-six months, the quality of erections often fades. Neither option is a winner here, and anyone telling you otherwise is likely selling you something. The choice then becomes: do you want the "cliff" of surgery or the "slope" of radiation? It is a grim calculation that we have to face honestly.
Busting the myths of the prostatectomy versus radiation debate
The problem is that many patients operate under the delusion that surgery is the only way to truly "get it out" and be done with the malignancy forever. Surgical extirpation certainly offers a tangible sense of closure because the organ physically exits the building. Let's be clear: removing the tissue does not magically grant a zero percent recurrence rate. Micrometastatic disease can lurk beyond the reach of the scalpel, which explains why biochemical recurrence occurs in approximately 20% to 40% of men within a decade of their operation. Because the biology of the tumor dictates the outcome more than the steel of the blade, the "clean slate" narrative is often a seductive oversimplification.
The radiation seeding fallacy
You might hear whispers in waiting rooms that radiation therapy turns your pelvic floor into a "nuclear wasteland" making future salvage surgery impossible. While fibrosis after high-dose photon delivery does complicate subsequent surgical planes, modern Stereotactic Body Radiotherapy (SBRT) uses such pinpoint accuracy that the collateral damage is significantly mitigated. It is not an all-or-nothing destruction. It is a calculated biological neutralizer. Yet, the fear of "secondary cancers" caused by the beams persists, despite the absolute risk being exceptionally low, often cited at less than 1% over a twenty-year horizon.
The potency paradox
Another misconception involves the timeline of sexual dysfunction. Surgery tends to hit the "off" switch immediately, with a potential—though never guaranteed—gradual recovery of erectile function over eighteen months if nerves were spared. Radiation takes the scenic route. It might preserve function initially, giving you a false sense of security, only for endarteritis obliterans to slowly choke off blood flow years down the line. Is it better to lose it all at once or watch it fade like a sunset? (A grim choice, perhaps, but one that requires honest expectations.) In short, neither path is a free pass for your libido.
The hidden variable: The "decisional regret" phenomenon
We rarely talk about the psychological weight of the choice itself. Choosing between removing prostate by surgery or radiation isn't just a medical toggle; it is a permanent lifestyle gamble. The issue remains that men who undergo surgery report higher rates of regret regarding urinary incontinence, while those who chose the beams worry more about long-term rectal irritation or "proctitis." External Beam Radiation Therapy (EBRT) involves a commitment to daily sessions for weeks, or five intense bursts in SBRT, whereas the surgeon’s robot finishes the job in a few hours. The time investment matters more than you think.
The genomic blueprint
Let's look at the "Decipher" score or other genomic classifiers. This is the expert’s secret weapon. If your tumor has a high-risk molecular signature, the local choice between a knife and a beam might be secondary to the need for systemic intensification with hormone blockers. Except that many clinics still treat every prostate like a generic lump of coal. As a result: we are seeing a shift toward personalized biology where the "how" of the local treatment matters less than the "what" of the cellular aggression. If you aren't asking for a genomic test, you are fighting a ghost in the dark.
Frequently Asked Questions
Which option has a higher survival rate for localized cancer?
Data from the landmark ProtecT trial, which followed over 1,600 men for fifteen years, demonstrated that prostate cancer-specific mortality was extremely low for both groups, sitting at roughly 3%. Whether you choose a radical prostatectomy or radiotherapy, the likelihood of dying from the disease remains nearly identical in the first decade and a half. The ProtecT study highlighted that while surgery reduced the risk of metastasis slightly more than active monitoring, the gap between surgery and radiation was statistically negligible. Consequently, your survival depends more on the Gleason score and initial staging than the specific modality of local destruction. You are choosing your side effects, not your expiration date.
How long is the recovery period for each treatment?
Surgery typically requires a catheter for seven to fourteen days and a physical activity restriction of about six weeks to prevent hernias or wound issues. Radiation allows you to keep working and maintain your routine, but the "fatigue wall" often hits around week three or four due to the cumulative cellular repair your body must perform. But the recovery isn't just about the first month; it’s about the year-long stabilization of your bladder and bowel habits. Men who opt for the robotic-assisted laparoscopic prostatectomy often find their "new normal" by six months, whereas radiation patients might face late-term changes years later. The issue remains that "recovery" is a moving target depending on your baseline health.
Will I definitely need hormone therapy with radiation?
Not necessarily, but for intermediate-risk or high-risk cases, adding Androgen Deprivation Therapy (ADT) for four to twenty-four months is the gold standard for improving outcomes. Studies indicate that combining beams with a temporary "testosterone fast" increases the biochemical-free survival rate significantly compared to radiation alone. If your physician suggests "short-term" ADT, it is because the hormones weaken the cancer cells, making the radiation twice as lethal. And it is important to remember that surgery rarely requires these drugs upfront, which is a major selling point for men who fear the hot flashes and muscle loss associated with low testosterone. Choosing between removing prostate by surgery or radiation often boils down to your willingness to tolerate these systemic temporary changes.
The definitive verdict on the pelvic crossroads
After navigating the murky waters of clinical data and patient anecdotes, one reality stands tall: the "best" treatment is the one that lets you sleep at night without mourning your quality of life. If you are a younger man with decades of life ahead, radical prostatectomy offers the most straightforward path for salvage options if the fire restarts later. For the older patient or those with significant comorbidities, radiation provides an elegant, non-invasive victory that preserves immediate function. I take the stance that surgery remains the superior choice for high-volume, healthy men because of the clarity provided by the pathology report, which no scan can perfectly mimic. We must stop pretending these choices are equal in experience just because they are equal in survival. You are not a statistic; you are a person who has to live with your bladder every single day. Trust the biology, but prioritize your anatomy.